
Fillable Printable 57.106 Psreportplan Blank
Fillable Printable 57.106 Psreportplan Blank
57.106 Psreportplan Blank
Form Approved
OMB No. 0920-0666
Exp. Date: 11/30/2019
www.cdc.gov/nhsn
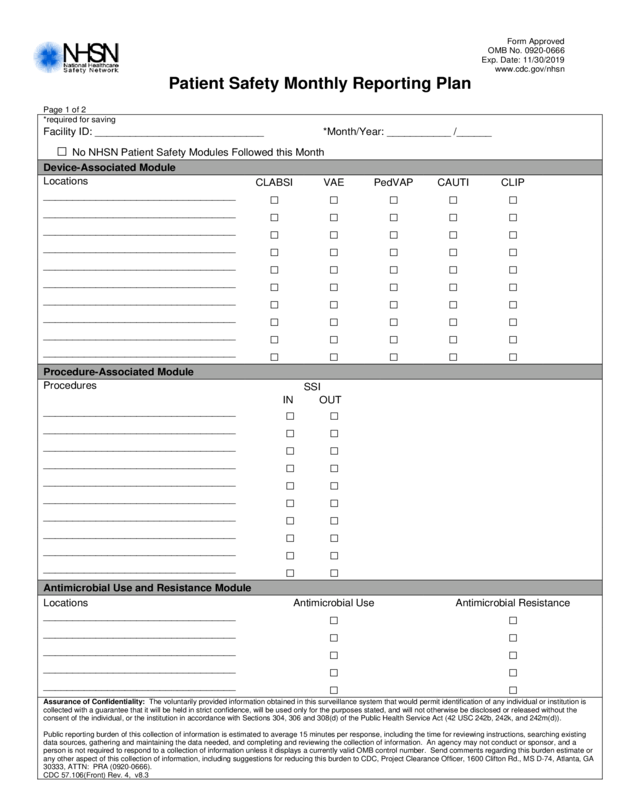
Patient Safety Monthly Re p orting Plan
Page 1 of 2
*required for saving
Facility ID: _____________________________ *Month/Year: ___________ /______
□ No NHSN Patient Safety Modules Followe d this Month
Device-Associated Module
Locations
CLABSI VAE PedVAP CAUTI CLIP
_________________________________
□ □ □ □ □
_________________________________
□ □ □ □ □
_________________________________
□ □ □ □ □
_________________________________
□ □ □ □ □
_________________________________
□ □ □ □ □
_________________________________
□ □ □ □ □
_________________________________
□ □ □ □ □
_________________________________
□ □ □ □ □
_________________________________
□ □ □ □ □
_________________________________
□ □ □ □ □
Procedure-Associated Modul e
Procedures
SSI
IN OUT
_________________________________
□ □
_________________________________
□ □
_________________________________
□ □
_________________________________
□ □
_________________________________
□ □
_________________________________
□ □
_________________________________
□ □
_________________________________
□ □
_________________________________
□ □
_________________________________
□ □
Antimicrobial Use and Resistance Module
Locations Antimicrobial Use Antimicrobial Resistance
_________________________________
□ □
_________________________________
□ □
_________________________________
□ □
_________________________________
□ □
_________________________________
□ □
Assurance of Confide nt iality: The voluntarily provided information obtained in this surveillance system that would permit identification of any individual or institution is
collected with a guarantee that it will be held in strict confidence, will be used only for the purposes stated, and will not otherwise be disclosed or released without the
consent of the individual, or the institution in accordance with Sections 304, 306 and 308(d) of the Public Health Service Act (42 USC 242b, 242k, and 242m(d)).
Public reporting burden of this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing
data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. An agency may not conduct or sponsor, and a
person is not required to respond to a collection of information unless it displays a currently valid OMB control number. Send comments regarding this burden estimate or
any other aspect of this collection of information, including suggestions for reducing this burden to CDC, Project Clearance Officer, 1600 Clifton Rd., MS D-74, Atlanta, GA
30333, ATTN: PRA (0920-0666).
CDC 57.106(Front) Rev. 4, v8.3
Form Approved
OMB No. 0920-0666
Exp. Date: 11/30/2019
www.cdc.gov/nhsn
CDC 57.106 (Back) Rev. 4, v8.3
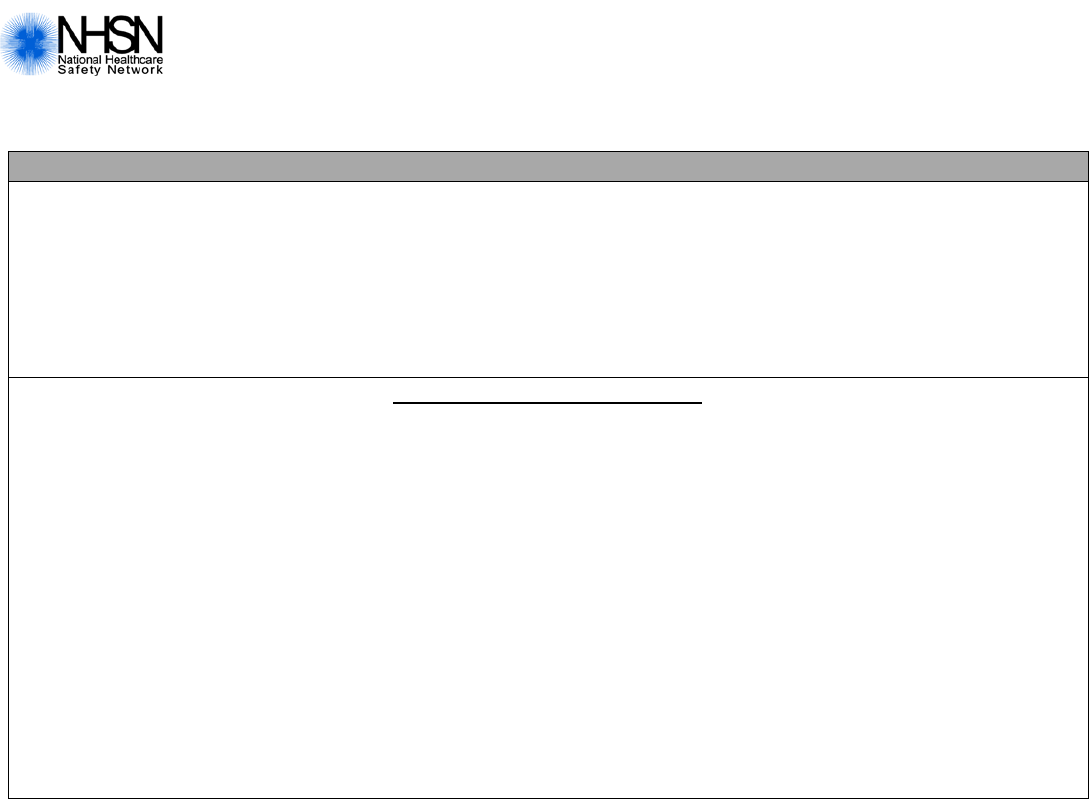
Patient Safety Monthly Reporting Plan
Page 2 of 2
MDRO and CDI Module
+Locations Specific Organism Type
±
LabID Event
±
LabID Event
(Circle one)
All Specimens Blood specimens only
FacWideIN FacWideOUT ______________
□ □
FacWideIN FacWideOUT ______________
□ □
FacWideIN FacWideOUT ______________
□ □
FacWideIN FacWideOUT ______________
□ □
Process and Outcom e Measures
Locations
Specific
Organism
Type
Infection
Surveillance
§
AST
Timing
§
AST
Eligible
Incidence Prevalence
LabID
Event
HH GG
__________ ________
□
Adm
Both
All
NHx
□ □ □ □ □
__________ ________
□
Adm
Both
All
NHx
□ □ □ □ □
__________ ________
□
Adm
Both
All
NHx
□ □ □ □ □
__________ ________
□
Adm
Both
All
NHx
□ □ □ □ □
__________ ________
□
Adm
Both
All
NHx
□ □ □ □ □
+ FacWideIN = Facility-wide Inpatient FacWideOUT = Facility-wide Outpatie nt
±
LabID Event = Laboratory-identified Event
§
For AST, circle on e choice to indicate time of t esting and one choice to indicate type of pati ents eligible for testing.
Timing: Adm = Admission Both = Both Admission and Discharge/Transfe r
Patients Eligibl e: All patients tested NHx = Only patients tested are those who have no documentation at the
admitting facility in the previous 12 months of MDRO-coloniz ation or infection
at the time of admissio n.


