
Fillable Printable 57.134 Pt Flu Vacc Standing Ord Blank
Fillable Printable 57.134 Pt Flu Vacc Standing Ord Blank
57.134 Pt Flu Vacc Standing Ord Blank
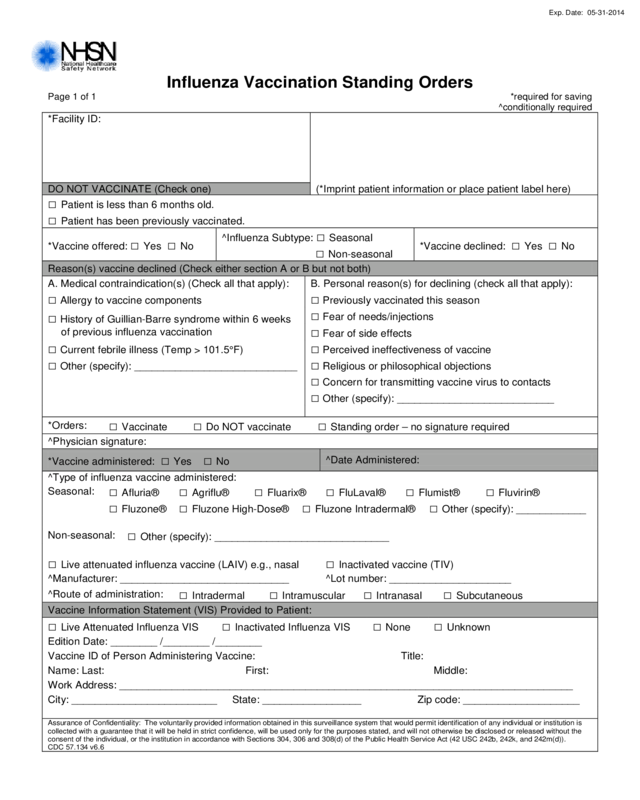
Influenza Vaccination Standing Orders
Page 1 of 1
*required for saving
^conditionally required
*Facility ID:
DO NOT VACCINATE (Check one)
(*Imprint patient information or place patient label here)
□ Patient is less than 6 months old.
□ Patient has been previously vaccinated.
*Vaccine offered: □ Yes □ No
^Influenza Subtype:
□
Seasonal
□ Non-seasonal
*Vaccine declined: □ Yes □ No
Reason(s) vaccine declined (Check either section A or B but not both)
A. Medical contraindication(s) (Check all that apply):
B. Personal reason(s) for declining (check all that apply):
□ Allergy to vaccine components
□ Previously vaccinated this season
□ History of Guillian-Barre syndrom e within 6 weeks
of previous influenza vaccination
□ Fear of needs/injections
□ Fear of side effects
□ Current febrile illness (Temp > 101.5°F)
□ Perceived ineffectiveness of vaccine
□ Other (specify): ____________________________
□ Religious or philosophical objections
□ Concern for transmitting vaccine virus to contacts
□ Other (specify): ___________________________
*Orders:
□ Vaccinate
□ Do NOT vaccinate
□ Standing order – no signature required
^Physician signature:
*Vaccine administered: □ Yes □ No
^Date Adm inister e d:
^Type of influenza vaccine administered:
Seasonal:
□ Afluria®
□ Agriflu®
□ Fluarix®
□ FluLaval®
□ Flumist®
□ Fluvirin®
□ Fluzone®
□ Fluzone High-Dose®
□ Fluzone Intradermal®
□ Other (specify): ____________
Non-seasonal:
□ Other (specify): ______________________________
□ Live attenuated influenza vaccine (LAIV) e.g., nasal
□ Inactivated vaccine (TIV)
^Manufacturer: _____________________________
^Lot number: _____________________
^Route of administration:
□ Intradermal
□ Intramuscular
□ Intranasal
□ Subcutaneous
Vaccine Information Statement (VIS) Provided to Patient:
□ Live Attenuated Influenza VIS
□ Inactivated Influenza VIS
□ None
□ Unknown
Edition Date: ________ /________ /________
Vaccine ID of Person Administering Vaccine: Title:
Name: Last:
First:
Middle:
Work Address: ______________________________________________________________________________
City: _________________________
State: _________________
Zip code: ____________________
Assurance of Confidentiality: The voluntarily provided information obtained in this surveillance system that would permit identi ficat i on of an y indi v idu al or ins ti tution is
collected with a guarantee that it will be held in strict confidence, will be used only for the purposes stated, and will not otherwise be disclosed or released without the
consent of the individual, or the institution in accordance with Sections 304, 306 and 308(d) of the Public Health Service Act (4 2 USC 24 2b, 242k, and 242m(d)).
CDC 57.134 v6.6
Exp. Date: 05-31-2014


