
Fillable Printable 57.205 Expbbf Blank
Fillable Printable 57.205 Expbbf Blank
57.205 Expbbf Blank
Form Approved
OMB No. 0920-0666
Exp. Date: 11/30/2019
www.cdc.gov/nhsn
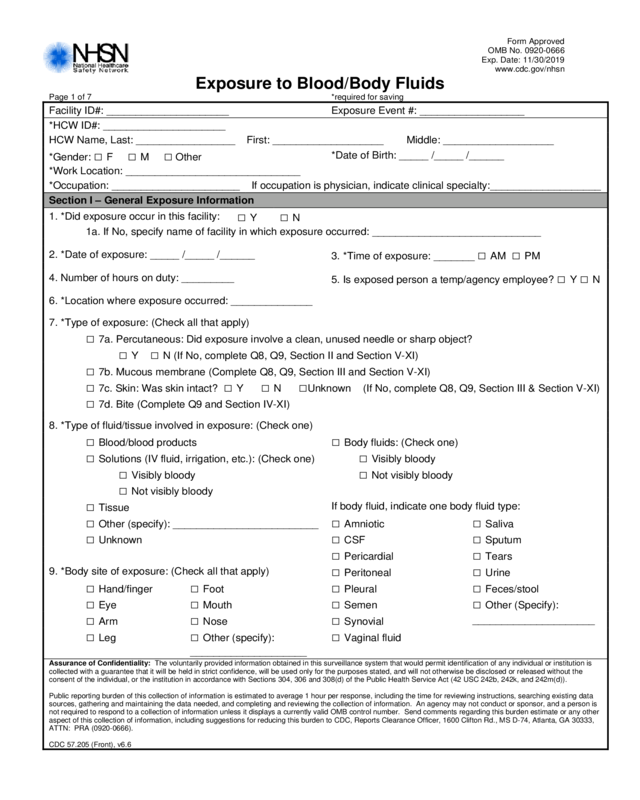
Exposure to Blood/Body Fl ui d s
Page 1 of 7 *required for saving
Facility ID#: _____________________ Exposure Event #: __________________
*HCW ID#: _____________________
HCW Name, Last: _________________ First: __________ _________ Middle: ___________________
*Gender: □ F □ M □ Other
*Date of Birth: _____ / _____ /______
*Work Location: ______________________________
*Occupation: ______________________ If occupation is physician, indicate clinical specialty:___________________
Section I – General Exposure Information
1. *Did exposure occ ur i n this facility:
□ Y □ N
1a. If No, specify nam e of facility in which exposure occurred: _____________________________
2. *Date of exposure: _____ /_____ /___ ___
3. *Time of exposure: _______
□ AM □ PM
4. Number of hours on duty: _________
5. Is exposed person a temp/agency em pl oyee?
□ Y □ N
6. *Location where exposure occurred: ______________
7. *Type of exposure: (Check all that apply)
□ 7a. Percutaneous: Did exposure involv e a clean, unused needle or sh arp object?
□ Y □ N (If No, complete Q8, Q9, Sect i on II and Section V-XI)
□ 7b. Mucous membran e (Complete Q8, Q9, Sect ion III and Section V -XI)
□ 7c. Skin: Was skin intact? □ Y □ N □Unknown (If No, complete Q8, Q9, S ect ion III & Section V-XI)
□ 7d. Bite (Complete Q9 and Section IV-XI)
8. *Type of fluid/tiss ue i nvolved in exposur e: (C heck one)
□ Blood/blood products □ Body fluids: (Chec k one)
□ Solutions (IV fluid, irrigation, etc.): (Check one) □ Visibly bloody
□ Visibly bloody □ Not visibly bloody
□ Not visibly bloody
□ Tissue
If body fluid, indicate one body fluid type:
□ Other (specify): ______ ________ ___ ____ ____ □ Amniotic □ Saliva
□ Unknown □ CSF □ Sputum
□ Pericardial □ Tears
9. *Body site of exposure: (Check all that appl y)
□ Peritoneal □ Urine
□ Hand/finger □ Foot □ Pleural □ Feces/stool
□ Eye □ Mouth □ Semen □ Other (Specify):
□ Arm □ Nose □ Synovial
_____________________
□ Leg □ Other (specify): □ Vaginal fluid
____________________
Assurance of Confide nt iality: The voluntarily provided information obtained in this surveillance system that would permit identification of any individual or institution is
collected with a guarantee that it will be held in strict confidence, will be used only for the purposes stated, and will not otherwise be disclosed or released without the
consent of the individual, or the institution in accordance with Sections 304, 306 and 308(d) of the Public Health Service Act (42 USC 242b, 242k, and 242m(d)).
Public reporting burden of this collection of information is estimated to average 1 hour per response, including the time for reviewing instructions, searching existing data
sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. An agency may not conduct or sponsor, and a person is
not required to respond to a collection of information unless it displays a currently valid OMB control number. Send comments regarding this burden estimate or any other
aspect of this collection of information, including suggestions for reducing this burden to CDC, Reports Clearance Officer, 1600 Clifton Rd., MS D-74, Atlanta, GA 30333,
ATTN: PRA (0920-0666).
CDC 57.205 (Front), v6.6
Form Approved
OMB No. 0920-0666
Exp. Date: 11/30/2019
www.cdc.gov/nhsn
CDC 57.205 (Back), v6.6
Exposure to Blood/Body Fluids
Page 2 of 7
Section II – Percutaneous Injury
1. *Was the needle o r sharp object visibl y contaminated with blood prior to exposure? □ Y □ N
2. Depth of the injury: (Check one)
□ Superficial, surface scratch □ Deep puncture or wound
□ Moderate, penetrated sk in □ Unknown
3. What needle or sharp object caused the inj ury (Check one)
□ Device (select one) □ Non-device sharp object (specify): ___________________ □ Unknown sharp object
Hollow-bore needle
□ Arterial blood coll ect ion device □ Biopsy needle □ Bone marrow needle
□ Hypodermic needle, attached to
syringe
□ Hypodermic needle, attached to IV
tubing
□ Unattached hypodermic needle
□ IV catheter – central line □ IV catheter – peripheral line □ Huber needle
□ Prefilled cartridge syrin ge □ IV stylet □ Spinal or epidural needle
□ Hemodialysis needle □ Dental aspirating syringe w/ needle □ Vacuum tube holder/ne edle
□ Winged-steel (Butterfly™ type)
needle
□ Hollow-bore needle, ty pe unknown □ Other hollow-bore needle
Suture needle
□ Suture needle
Other solid sharps
□ Bone cutter □ Bur □ Electrocautery device
□ Elevator □ Explorer □ Extraction forceps
□ File □ Lancet □ Microtome blade
□ Pin □ Razor □ Retractor
□ Rod (orthopedic) □ Scaler/curette □ Scalpel blade
□ Scissors □ Tenaculum □ Trocar
□ Wire
Glass
□ Capillary tube □ Blood collection tube □ Medication ampule/v i al /bottle
□ Pipette □ Slide □ Specimen/test/ vacuum tube
Plastic
□ Capillary tube □ Blood collection tube □ Specimen/test/ vacuum tube
Non-sharp saf ety device
□ Blood culture adapte r □ Catheter securement device □ IV delivery system
□ Other known device (specify): _________________________________
4. Manufacturer and Model: _____________________________________
Form Approved
OMB No. 0920-0666
Exp. Date: 11/30/2019
www.cdc.gov/nhsn
CDC 57.205 (Back), v6.6
Exposure to Blood/Body Fluids
Page 3 of 7
5. Did the needle or other sharp object involved in the injury have a safety feature? □ Y □ N
5a. If Yes, indicate t ype of safety feature: (Check one) If No, skip to Q6.
□ Bluntable needle, sharp □ Needle/sharp eject or
□ Hinged guard/shield □ Mylar wrapping/pla sti c
□ Retractable needl e/sharp □ Other safety f eature (specify):____________________
□ Sliding/gliding gua rd/ shield □ Unknown safety mechanism
5b. If the device had a safety feature, when did the injury occur? (Check one)
□ Before activation of the safety feature was
appropriate
□ Safety feature failed, af ter activation
□ During activat ion of the safety feature □ Safety feature not acti vated
□ Safety feature improp erly activated □ Other (specify): ______ ________ ___ ____ _______ _
6. When did the injury occur? (Check one)
□ Before use of the item □ During or after disp osal
□ During use of the it em □ Unknown
□ After use of the item before disposal
7. For what purpose or activity was the sharp d evice being used? (Che ck one)
Obtaining a blood s pecimen percutaneo usly
□ Performing phlebotomy □ Performing a fingerstick/heelstick
□ Performing arterial puncture □ Other blood-sampli ng procedure
(specify): ______________________ _____________
Giving a percutaneo us injection
□ Giving an IM injection □ Placing a skin test (e. g., tuberculin, allergy, etc.)
□ Giving a SC injection
Performing a line related procedure
□ Inserting or withdrawing a catheter □ Injecting into a line or po rt
□ Obtaining a blood sample from a central or
peripheral I.V. line or port
□ Connecting an I.V. line
Performing surgery/autopsy/other invasive procedure
□ Suturing □ Palpating/exploring
□ Incising □ Specify procedure: ____________________________
Performing a dental procedure
□ Hygiene (prophylaxis) □ Oral surge ry
□ Restoration (amalgam composite, crown) □ Simple extraction
□ Root canal □ Surgical extraction
□ Periodontal surgery
Handling a specimen
□ Transferring B B F i nto a specimen container □ Processing specimen
Other
□ Other diagnosti c procedure (e.g., t horacentesis) □ Unknown
□ Other (specify): ______ ________ ___ ____ _______
Form Approved
OMB No. 0920-0666
Exp. Date: 11/30/2019
www.cdc.gov/nhsn
CDC 57.205 (Back), v6.6
Exposure to Blood/Body Fluids
Page 4 of 7
8. What was the activit y at the time of injury? (Check one)
□ Cleaning room □ Collecting/transpo rti ng waste
□ Decontamination/ processing used equi pm ent □ Disassembling device/equipment
□ Handling equipment □ Opening/breaking glass container (e.g. , ampule)
□ Performing procedu re □ Placing sharp in container
□ Recapping □ Transferring/passing/recei ving device
□ Other (specify): ______ ________ ___ ____ _______ ____ ____ _
9. Who was holding the d evice at the time the i nj ury occurred? (Chec k one)
□ Exposed person
□ Co-worker/other pe rson
□ No one, the sharp was an uncontrolled sharp in the environment
10. What happene d when the injury occurred? ( Check one)
□ Patient moved and jarred device □ Contact with overfil l ed/punctured shar ps c ontainer
□ Device slipped □ Improperly di sposed sharp
□ Device rebounded □ Other (specify): _______________________________
□ Sharp was being reca pped □ Unknown
□ Collided with co-work er or other person
Form Approved
OMB No. 0920-0666
Exp. Date: 11/30/2019
www.cdc.gov/nhsn
CDC 57.205 (Back), v6.6
Exposure to Blood/Body Fluids
Page 5 of 7
Section III – Mucous Membrane and/or Skin Exposure
1. Estimate the amount of blood/body fluid exposure: (Chec k one)
□ Small (<1 tsp or 5cc) □ Large (> ¼ cup or 50cc)
□ Moderate (>1 tsp and up to ¼ cup, or 6-50 cc) □ Unknown
2. Activity/event when exposure occ urred: (Check one)
□ Airway manipulation (e.g., suctioning ai rway ,
inducing sputum)
□ Patient spit/cough ed/vomited
□ Bleeding vessel □ Phlebotomy
□ Changing dressing/w ound care
□ Surgical procedur e (e. g., all surgical procedures
including C-section)
□ Cleaning/transporting contaminated equipment
□ Tube placement/rem oval/manipulation (e.g., chest,
endotracheal, NG, rectal, urine catheter)
□ Endoscopic procedures □ Vaginal delivery
□ IV or arterial line insert ion/removal/manipulation □ Other (specify): ______ ________ ___ ____ _______ ___
□ Irrigation procedu res □ Unknown
□ Manipulating bloo d t ube/bottle/speci m en
container
3. Barriers used by the worker at the time of exposure: (Check all that appl y)
□ Face shield □ Mask/respirator
□ Gloves □ Other (specify): ______ ________ ___ ____ _______ ___
□ Goggles □ No barriers
□ Gown
Section IV – Bite
1. Wound description: (Check one)
□ No spontaneous bleeding □ Tissue avulsed
□ Spontaneous bleeding □ Unknown
2. Activity/event when exposure occ urred: (Check one)
□ During dental procedure □ Assault by patient
□ During oral examination □ Other (specify): ______ ________ ___ ____ _______ ___
□ Providing oral hygiene □ Unknown
□ Providing non-oral care t o pat i ent
Form Approved
OMB No. 0920-0666
Exp. Date: 11/30/2019
www.cdc.gov/nhsn
CDC 57.205 (Back), v6.6
Exposure to Blood/Body Fluids
Page 6 of 7
Note: Section V-IX are required when following the protocols for Exposure Management.
Section V – Source Information
1. Was the source patient known? □ Y □ N
2. Was HIV status known at the time of exposure? □ Y □N
3. Check the test re sult s f or the source patient (P=positive, N=negative, I=indeterm inate, U=unknown, R=refused, NT=not t est ed)
Hepatitis B P N I U R NT
HBsAg
HBeAg
Total anti-HBc
Anti-HBs
Hepatitis C
Anti-HCV EIA
Anti-HCV supplemental
PCR-HCV RNA
HIV
EIA, ELISA
Rapid HIV
Confirmatory test
Section VI – For HIV Infected Source
1. Stage of disease: (Check one)
□ End-stage AIDS □ Other symptomatic HIV, not AIDS
□ AIDS □ HIV infection, no symptoms
□ Acute HIV illness □ Unknown
2. Is the source patient taking anti-ret roviral drugs? □ Y □ N □ U
2a. If yes, indicate drug(s): __________ __________ __________ __________ __________ __________
3. Most recent CD4 count : ________mm
3
Date: ____ /______ (mo/ yr)
4. Viral load: _____ copies/ml _____ undetectable Date: ____ /______ (mo/yr)
Section VII – Initial Care Given to Healthcare Worker
1. HIV postexpos ure prophylaxis:
Offered? □ Y □ N □ U Taken: □ Y □ N □ U (If Yes, complete PEP form)
2. HBIG given? □ Y □ N □ U
Date administered: ____ /____ /______ _
3. Hepatitis B v accin e given: □ Y □ N □ U
Date 1
st
dose administered: ____ /____ /____ ___
4. Is the HCW pregnant? □ Y □ N □ U
4a. If yes, which trimester? □ 1 □ 2 □ 3 □ U
Form Approved
OMB No. 0920-0666
Exp. Date: 11/30/2019
www.cdc.gov/nhsn
CDC 57.205 (Back), v6.6
Exposure to Blood/Body Fluids
Page 7 of 7
Section VIII – Baseline Lab Testing
Was baseline testing performed on the H CW ? □ Y □ N □ U If Yes, indicate results
Test Date Result Test Date Result
HIV EIA __ /__ /____ P N I R ALT __ /__ /____ ____ IU/L
HIV Confirmatory __ /__ /____ P N I R Amylase __ /__ /____ ____ IU/L
Hepatitis C anti-HCV-EIA __ /__ /____ P N I R Blood glucose __ /__ /____ ____ mmol/L
Hepatitis C anti-HCV-supp __ /__ /____ P N I R Hematocrit __ /__ /____ ____ %
Hepatitis C PRC HCV RNA __ /__ /____ P N I Hemoglobin __ /__ /____ ____ gm/L
Hepatitis B HBs Ag __ /__ /____ P N I Platelets __ /__ /____ ____ x10
9
/L
Hepatitis B IgM anti-HBc __ /__ /____ P N I Blood cells in Urine __ /__ /____ ____ #/mm
3
Hepatitis B Total anti-HBc __ /__ /____ P N I WBC __ /__ /____ ____ x10
9
/L
Hepatitis B Anti-HBs __ /__ /____ _____ mIU/mL Creatinine __ /__ /____ ____ μmol/L
Result Codes: P=Positive, N=Negative, I=Indeterminate, R=Refused
Other: __________ __ /__ /____ ___________
Section IX – Follow-up
1. Is it recommended that the HCW return f or f ol l ow-up of this exposur e? □ Y □ N
1a. If Yes, will follow-up be performed at this facility? □ Y □ N
Section X – Narrative
In the worker’s words, how did the injury occur?
Section XI – Prevention
In the worker’s words, what could have prevented the injury?
Custom Fields
Label Label
_________________________ ____/____/_____ _________________________ ____/____/_____
_________________________ ______________ _________________________ ______________
_________________________ ______________ _________________________ ______________
_________________________ ______________ _________________________ ______________
_________________________ ______________ _________________________ ______________
_________________________ ______________ _________________________ ______________
Comments


