
Fillable Printable 57.207 Labtesting Blank
Fillable Printable 57.207 Labtesting Blank
57.207 Labtesting Blank
Form Approved
OMB No. 0920-0666
Exp. Date: 11/30/2019
www.cdc.gov/nhsn
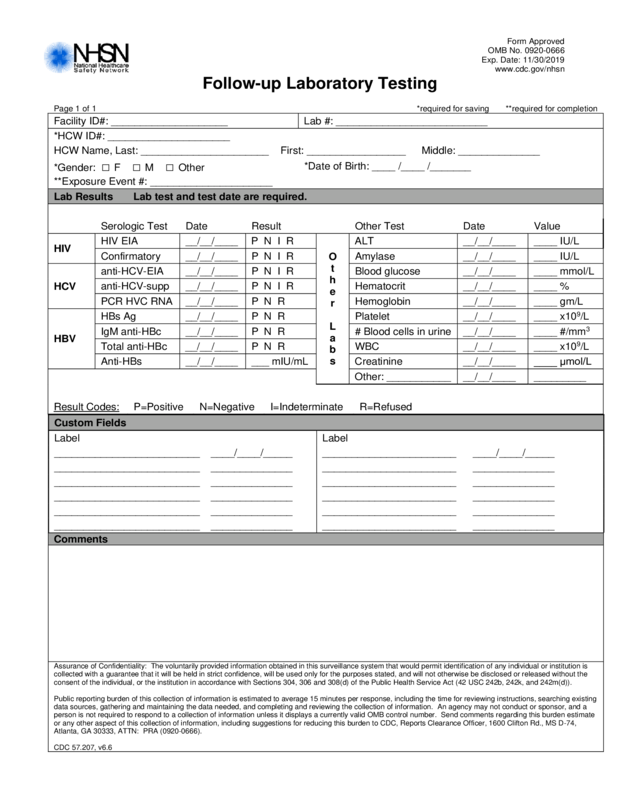
Follow-up Laboratory Tes ti n g
Page 1 of 1 *required for saving **required for completion
Facility ID#: ____________________ Lab #: __________________________
*HCW ID#: _____________________
HCW Name, Last: ______________________ First: _________________ Middle: ________ ______
*Gender: □ F □ M □ Other
*Date of Birth: ____ / ____ /_______
**Exposure Ev ent #: ________________ _____
Lab Results Lab test and test date are required.
Serologic Test Date Result
Other Test Date Value
HIV
HIV EIA __/__/____ P N I R
O
t
h
e
r
L
a
b
s
ALT __/__/____
____ IU/L
Confirmatory __/__/____ P N I R Amylase __/__/____ ____ IU/L
HCV
anti-HCV-EIA __/__/____
P N I R Blood glucose __/__/____ ____ mmol/L
anti-HCV-supp __/__/____ P N I R Hematocrit __/__/____ ____ %
PCR HVC RNA __/__/____ P N R Hemoglobin __/__/____ ____ gm/L
HBV
HBs Ag __/__/____
P N R Platelet __/__/____ ____ x10
9
/L
IgM anti-HBc __/__/____ P N R # B l ood cells in urine __/__/____ ____ #/mm
3
Total anti-HBc __/__/____ P N R WBC __/__/____ ____ x10
9
/L
Anti-HBs __/__/____ ___ mI U/ m L Creatinine __/__/____ ____ μmol/L
Other: ___________ __/__/____ _________
Result Codes: P=Positive N=Negative I=Indeterminate R=Refused
Custom Fields
Label Label
_________________________ ____/____/_____ _______________________ ____/____/_____
_________________________ ______________ _______________________ ______________
_________________________ ______________ _______________________ ______________
_________________________ ______________ _______________________ ______________
_________________________ ______________ _______________________ ______________
_________________________ ______________ _______________________ ______________
Comments
Assurance of Confidentiality: The voluntarily provided information obtained in this surveillance system that would permit identification of any individual or institution is
collected with a guarantee that it will be held in strict confidence, will be used only for the purposes stated, and will not otherwise be disclosed or released without the
consent of the individual, or the institution in accordance with Sections 304, 306 and 308(d) of the Public Health Service Act (42 USC 242b, 242k, and 242m(d)).
Public reporting burden of this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing
data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. An agency may not conduct or sponsor, and a
person is not required to respond to a collection of information unless it displays a currently valid OMB control number. Send comments regarding this burden estimate
or any other aspect of this collection of information, including suggestions for reducing this burden to CDC, Reports Clearance Officer, 1600 Clifton Rd., MS D-74,
Atlanta, GA 30333, ATTN: PRA (0920-0666).
CDC 57.207, v6.6


