
Fillable Printable Acute Mapping Matrix
Fillable Printable Acute Mapping Matrix
Acute Mapping Matrix
Reporting Guide For Acute Health Care Contractors
Revenue and Expense Statement Mapping Guidelines
Updated August, 2016 1
\\snas01\s-drive.DHCM\FIN\Reporting Guide\CYE 17\Acute\Final documents\Acute Mapping Matrix.docx\\snas01\s-drive.DHCM\FIN\Reporting Guide\CYE
17\Acute\Final documents\Acute Mapping Matrix.docx
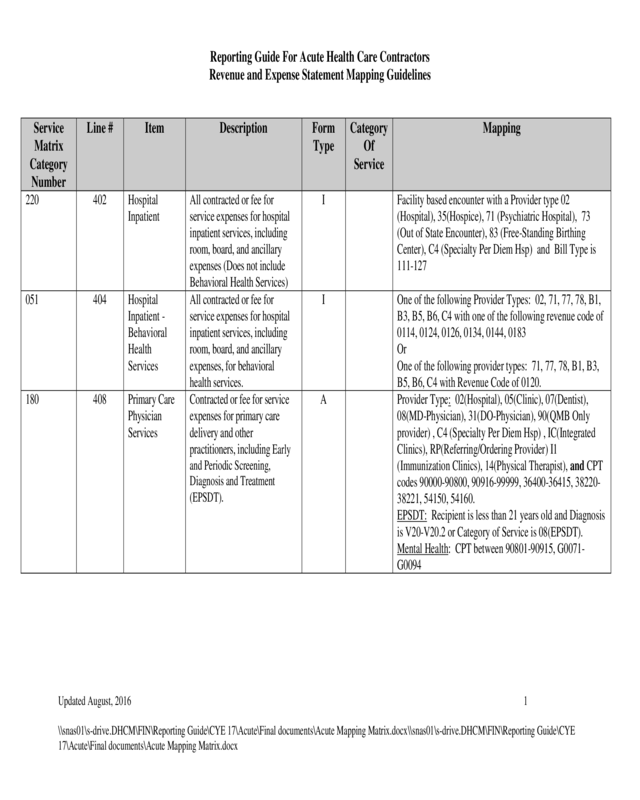
Service
Matrix
Category
Number
Line #
Item
Description
Form
Type
Category
Of
Service
Mapping
220
402
Hospital
Inpatient
All contracted or fee for
service expenses for hospital
inpatient services, including
room, board, and ancillary
expenses (Does not include
Behavioral Health Services)
I
Facility based encounter with a Provider type 02
(Hospital), 35(Hospice), 71 (Psychiatric Hospital), 73
(Out of State Encounter), 83 (Free-Standing Birthing
Center), C4 (Specialty Per Diem Hsp) and Bill Type is
111-127
051
404
Hospital
Inpatient -
Behavioral
Health
Services
All contracted or fee for
service expenses for hospital
inpatient services, including
room, board, and ancillary
expenses, for behavioral
health services.
I
One of the following Provider Types: 02, 71, 77, 78, B1,
B3, B5, B6, C4 with one of the following revenue code of
0114, 0124, 0126, 0134, 0144, 0183
Or
One of the following provider types: 71, 77, 78, B1, B3,
B5, B6, C4 with Revenue Code of 0120.
180
408
Primary Care
Physician
Services
Contracted or fee for service
expenses for primary care
delivery and other
practitioners, including Early
and Periodic Screening,
Diagnosis and Treatment
(EPSDT).
A
Provider Type: 02(Hospital), 05(Clinic), 07(Dentist),
08(MD-Physician), 31(DO-Physician), 90(QMB Only
provider) , C4 (Specialty Per Diem Hsp) , IC(Integrated
Clinics), RP(Referring/Ordering Provider) I1
(Immunization Clinics), 14(Physical Therapist), and CPT
codes 90000-90800, 90916-99999, 36400-36415, 38220-
38221, 54150, 54160.
EPSDT: Recipient is less than 21 years old and Diagnosis
is V20-V20.2 or Category of Service is 08(EPSDT).
Mental Health: CPT between 90801-90915, G0071-
G0094
Reporting Guide For Acute Health Care Contractors
Revenue and Expense Statement Mapping Guidelines
Updated August, 2016 2
\\snas01\s-drive.DHCM\FIN\Reporting Guide\CYE 17\Acute\Final documents\Acute Mapping Matrix.docx\\snas01\s-drive.DHCM\FIN\Reporting Guide\CYE
17\Acute\Final documents\Acute Mapping Matrix.docx
Service
Matrix
Category
Number
Line #
Item
Description
Form
Type
Category
Of
Service
Mapping
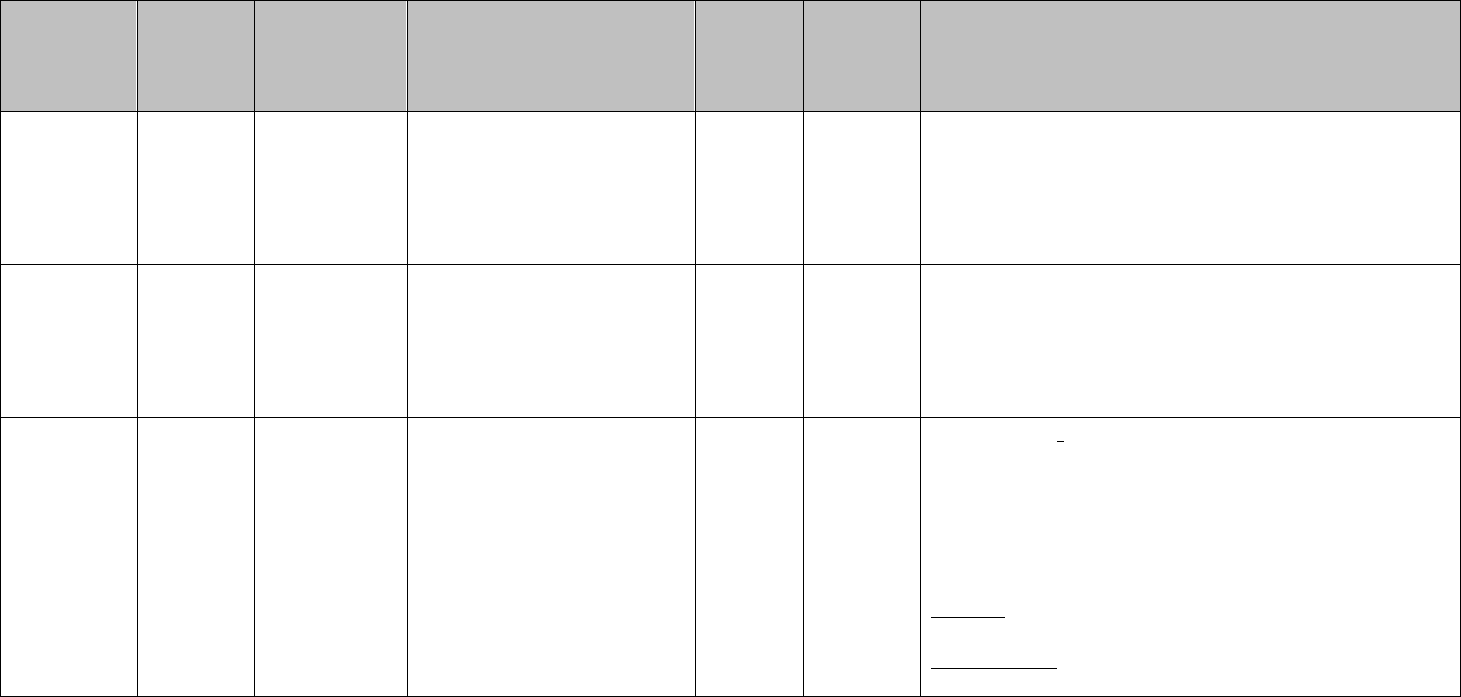
052
409
Behavioral
Health
Physician
Services
Expenses for physician
services related to Behavioral
Health services.
A
Provider type 11, 39, 77, 85, 86, 87, A2, A3, A4, A5, A6
Select by provider type or AHCCCS COS with HCPCS
codes equal to: H0001, H0002, H0003, H0004, H0017,
H0018, H0019, H0025, H0031, H0034, H0038, H2000,
H2011, H2012, H2014, H2015, H2016, H2017, H2019,
H2020, H2025, H2027, S5110, T1002, T1016, T1019,
T1020, 90801, 90802, 90804, 90805, 90806, 90807,
90808, 90809, 90810, 90811, 90812, 90813, 90814,
90815, 90816, 90817, 90818, 90819, 90821, 90822,
90823, 90824, 90826, 90827, 90828, 90829, 90845,
90846, 90847, 90849, 90853, 90857, 90862, 90865,
90870, 90875, 90876, 90880, 90882, 90885, 90887,
90889, 90899, 96101, 96102, 96103, 96105, 96110,
96111, 96116, 96118, 96119, 96120, 96125, 96150,
96151, 96152, 96153, 96154, 96155, 99255, H0020 with
modifier equal to HG, H2010 with modifier equal to HG
Select by HCPCS codes: 99201-99499 (if not previously
selected by Service Matrix Category 40- Primary Care
Service)
Select by HCPCS H0020 and H2010 both codes with
modifier equal to HG
160, 170
410
Referral
Physician
Services
Contracted or fee for service
expenses for referral
(specialist) physician services.
This is Surgery and OB/GYN
Services
A
Provider Type: 02(Hospital), 05(Clinic), 07(Dentist),
08(MD-Physician), 31(DO-Physician), C4 (Specialty Per
Diem Hsp), 14 (Physical Therapist), 90 (QMB Only
Provider) also CPT 10000-69999 with COS 02 or 00100-
01999 with COS 01, 02.
Exclude 54150 and 54160(Circumcision) and T1015
Reporting Guide For Acute Health Care Contractors
Revenue and Expense Statement Mapping Guidelines
Updated August, 2016 3
\\snas01\s-drive.DHCM\FIN\Reporting Guide\CYE 17\Acute\Final documents\Acute Mapping Matrix.docx\\snas01\s-drive.DHCM\FIN\Reporting Guide\CYE
17\Acute\Final documents\Acute Mapping Matrix.docx
Service
Matrix
Category
Number
Line #
Item
Description
Form
Type
Category
Of
Service
Mapping
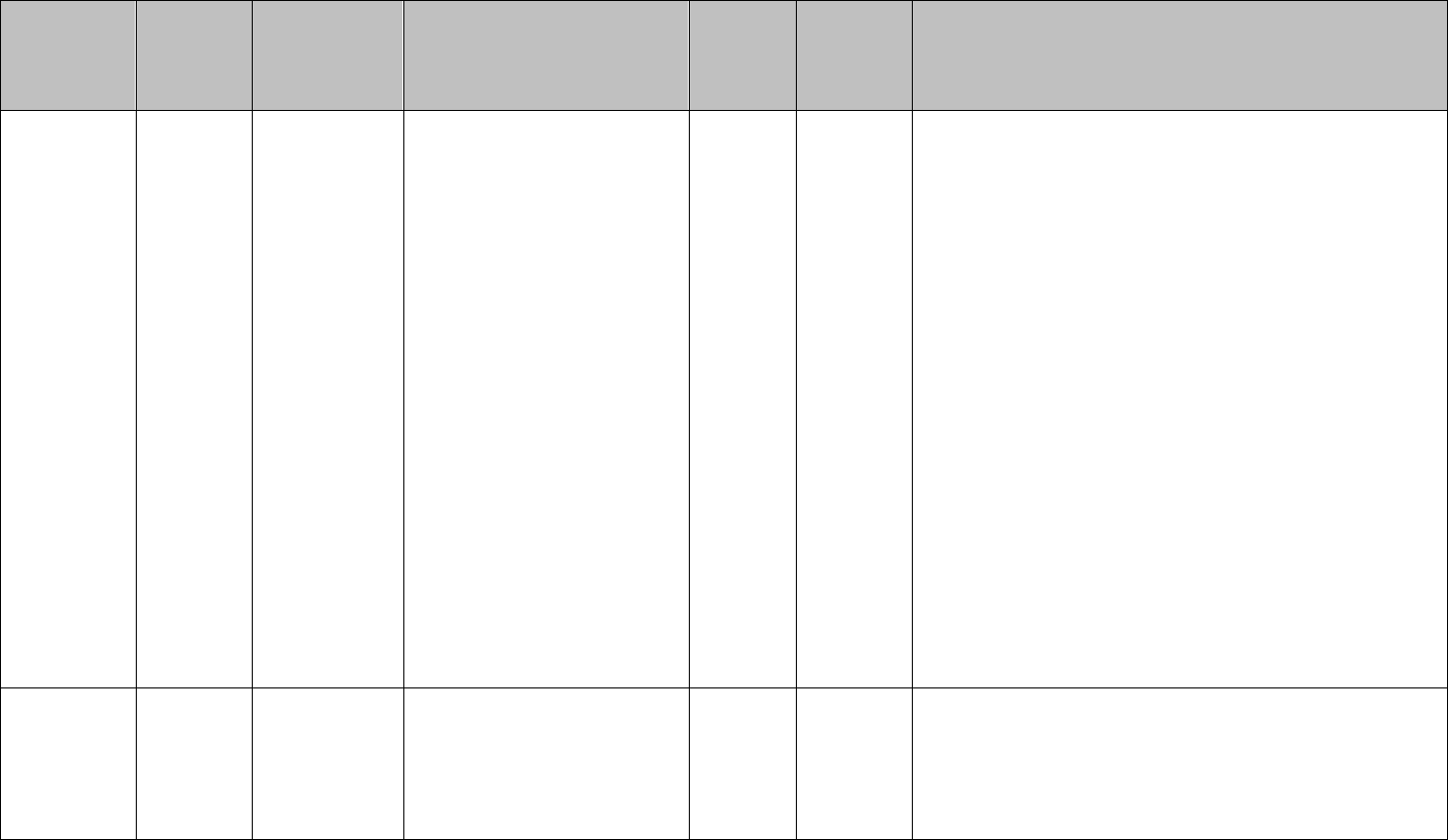
For OB/GYN services use 56405-59999 regardless of the
category of service. Also include the following diagnostic
codes: 614-677, V22.xx, V23.xx, V24.xx, V25.xx,
V27.xx, V28.xx, and V72.3x & V72.4X, providing both
form type and provider type conditions are met.
350
411
FQHC/RHC
Services
FQHC/RHC services should
be recorded to this line if the
services meet the definition of
a visit or are incidental to the
visit.
A or D
Provider type for FQHCs and FQHC Look-Alikes is C2
Provider type for RHCs is 29.
190
412
Other
Professional
Services
All other Professional
Services not otherwise
classified above (408-410).
A
Select all HCPCS/CPT Codes for the following provider
types: 03, 04, 09, 10, 11, 12, 13, 15, 16, 17, 18, 19, 22,
26, 30, 31 32, 36, 41, 46, 47, 48, 56, 62, 67, 68, 69, 73, 79,
82, 83, 84, 85, 86, 87, , E1, OR the category of service 45
for all services which have not already been mapped
elsewhere.
120
416
Emergency
Facility
Services
Those expenses relating to
emergency room and urgent
care facility services provided
on an outpatient basis.
O
Rev Code 450-459.
Only ER services that did not result in a hospital
admission will be counted in this category. Form type O
should limit this.
330
417
Pharmacy
Pharmacy expenses incurred
for outpatient services
C, O
Form Type O: Rev codes 250-259, 630-633, 636
Select if Claim Type = E (Encounter)
Select for all Form Type = C (Pharmacy)
110
418
Lab, X-ray and
Medical
Imaging
Pathology, Laboratory and
radiology (medical imaging,
x-ray) expenses incurred for
outpatient services
A
12 or 13
Also any other HCPCS that match the category of service
value.
Reporting Guide For Acute Health Care Contractors
Revenue and Expense Statement Mapping Guidelines
Updated August, 2016 4
\\snas01\s-drive.DHCM\FIN\Reporting Guide\CYE 17\Acute\Final documents\Acute Mapping Matrix.docx\\snas01\s-drive.DHCM\FIN\Reporting Guide\CYE
17\Acute\Final documents\Acute Mapping Matrix.docx
Service
Matrix
Category
Number
Line #
Item
Description
Form
Type
Category
Of
Service
Mapping
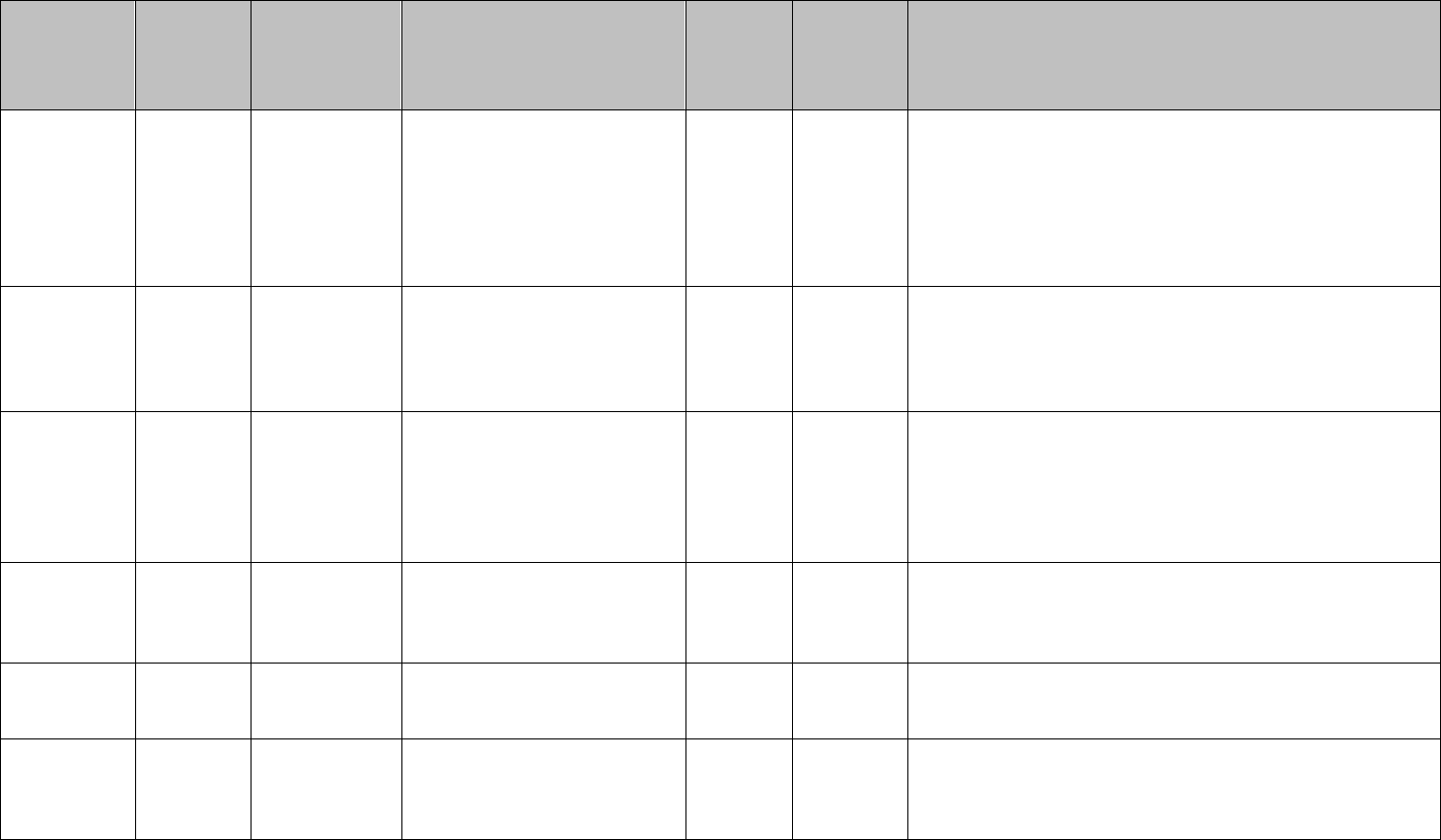
130
419
Outpatient
Facility
Outpatient facility expenses
incurred for outpatient
services. Includes
outpatient/ambulatory surgical
center.
O, A, I
Form type O rev codes not in the following ranges: 450-
459. Form type A with provider type of 43 (Ambulatory
Surgical Center). Do not include encounters only that
contain the following rev codes (These will be included in
Pharmacy): 250-259, 630-633, 636.
Form type I pay code OPF, and CCO. Pay code TIR with
Form Type 1 only when no tier levels found.
090
420
Durable
Medical
Equipment
Medical equipment, medical
supplies, medical appliances
and oxygen expenses incurred
for outpatient services.
A
15 or 40
For Rented: select by all HCPCS with AHCCCS Category
of Service values and modifier codes equal to NR, RR or
LL
For Purchased: select by all HCPCS with AHCCCS
Category of Service values. Bypass those selected in the
Rental Category
150
421
Dental
Dental expenses incurred for
outpatient services, including
outpatient surgery, pharmacy,
lab, and radiology specifically
related to a dental diagnosis.
D, A
11
Select all form type D and select form type A and COS 11
10, 20, 30,
40, 50,
60, 70, 80,
422
Transportation
Medically necessary
transportation expenses
incurred for inpatient and
outpatient services, both
emergency and non-
emergency.
A
HCPC Codes: A0021-A0999, Q3019, Q3020, S0209,
S0215, T2001-T2007, T2049, Z0030, Z2999, Z3344,
Z3620, Z3643, Z3655, Z3700
Total Emergency Trips – includes base, mileage, supplies
cost, and uses base unity quantity only.
Total Non-Emergency Trips – includes base, mileage,
miscellaneous costs above. Uses base unity quantity only.
Reporting Guide For Acute Health Care Contractors
Revenue and Expense Statement Mapping Guidelines
Updated August, 2016 5
\\snas01\s-drive.DHCM\FIN\Reporting Guide\CYE 17\Acute\Final documents\Acute Mapping Matrix.docx\\snas01\s-drive.DHCM\FIN\Reporting Guide\CYE
17\Acute\Final documents\Acute Mapping Matrix.docx
Service
Matrix
Category
Number
Line #
Item
Description
Form
Type
Category
Of
Service
Mapping
200, 210
423
Nursing
Facility (NF),
Home Health
Care
Expenses relating to nursing
facility (NF) and home health
care including durable medical
equipment expense incurred in
a NF or home health care
setting. Examples include:
Intermediate Care Facility and
Skilled Nursing Facility.
L, A
Nursing Facility: Form Type L
Home Health: Provider Type – 23(Home Health Agency),
24(Personal Care Attendant), 27(Adult Day Health),
36(Assisted Living Home), 37(Homemaker), 40(Attendant
Care), 46(Nurse-Private RN or LPN), 50(Adult Foster
Care), 57 (Residential treatment facility),70(Home
Delivered Meals) 95 (Non Medicare Certified Home
Health Agencies) or HCPC Codes: S5100, S5101, S5102,
S5125, S5130, S5140 S5150-HQ, S5151, S5165, S5170,
S9123, S9123-TG, S9124, S9124-TG, T1019, T1021,
T2016, T2017, T2018, T2019, T2021, T2026, T2031,
T2031-TF, T2031-TG, T2033, T2033-UI, TF, G0154
140
424
Physical
Therapy
Physical therapy and physical
rehabilitation incurred for
outpatient services.
A
06
Provider Type not equal to 02(Hospital), 05(Clinic),
08(MD-Physician), 31(DO-Physician Osteopath),
42(Hospital Affiliated Clinic) , C4 (Specialty Per Diem
Hsp) Select by all HCPCS that meet Provider Type and
AHCCCS Category of Service requirements.
BH Service
Matrix 001
426
Behavioral
Health Day
Program
Medical, Home and
Community expenses incurred
for services provided to
members in a Behavioral
Health Day Program including
supervised day program,
therapeutic day program, and
medical day program.
A
HCPCS codes H0036, H0036-TF, H0037, H2015, H2012,
H2019, H2019-TF, H2020
BH Service
Matrix 014
427
Behavioral
Health Case
Management
Case management expenses
related to behavioral health
services, including salaries,
A
HCPCS codes 90887, 90889, 98966, 98967, 98968,
99367, 99368, 99441- 99443, T1016-HN, HO, GT
Reporting Guide For Acute Health Care Contractors
Revenue and Expense Statement Mapping Guidelines
Updated August, 2016 6
\\snas01\s-drive.DHCM\FIN\Reporting Guide\CYE 17\Acute\Final documents\Acute Mapping Matrix.docx\\snas01\s-drive.DHCM\FIN\Reporting Guide\CYE
17\Acute\Final documents\Acute Mapping Matrix.docx
Service
Matrix
Category
Number
Line #
Item
Description
Form
Type
Category
Of
Service
Mapping
Services
benefits, travel, and training
expenses for the case
manager(s), and case
management supervisors
BH Service
Matrix 002
428
Behavioral
Health Crisis
Intervention
Services
Expenses incurred for Crisis
Intervention Services provided
to members including mobile,
stabilization and telephone.
A
HCPCS codes H2011, H2011- HT, 99281, 99282, 99283,
99284, 99285, S9484, S9485
BH Service
Matrix 012
429
Behavioral
Health
Rehabilitation
Services
Expenses incurred for
Rehabilitation Services
provided to members
including living skills training,
Cognitive Rehab, Health
Promotion, and Supported
Employment Services.
A
HCPCS codes 97532, H0025, H0034, H2014, H2014-
HK, H2014-HQ, H2017, H2025, H2026, H2027
BH Service
Matrix 013
430
Behavioral
Health
Residential
Services
Expenses incurred for
Residential Services provided
to members including Level II
and Level III Behavioral
Health Residential Facility
Room and Board.
A
HCPCS codes H0018, H0019,


