
Fillable Printable Appendix E Child Anxiety
Fillable Printable Appendix E Child Anxiety
Appendix E Child Anxiety
TOOL KIT
FOR THE MANAGEMENT OF
CHILDHOOD
&
ADOLESCENT
ANXIETY
This tool kit was developed by the AHCCCS Tool Kit Workgroup in collaboration with Acute Health Plans and ADHS/DBHS (January, 2008
through January, 2009). This tool kit is only a resource and may not apply to all patients and all clinical situations. It is not intended to replace
clinical judgment.
Initial Effective Date: 5/1/2009 Revision Date: 5/01/2011
TOOL KIT FOR THE MANAGE MENT OF
C
HILDHOOD & ADOLESCENT ANXIETY
The clinical tool kit is intended to assist the PCP in assessing the needs of the child/adolescent,
ranging in age from 8 through 18, regarding anxiety and decisions regarding health care services
provided by the PCP or subsequent referral to the Regional Behavioral Health Authority
(RBHA) if clinically indicated. Tools include:
• The decision making algorithm
• The “Anxiety Disorders In Adolescents: A Self Test” Document
• The “Anxiety Disorders in Children: A Test for Parents” Document
• The list of medications universally available through AHCCCS Health Plans and the
RBHA.
Clinical resources and adaptations of clinical sources are referenced within the individual
documents.
NOTE:
• Strongly consider referring children under 8 years old to the RBHA for treatment.
• A RBHA consultation is available at any time.
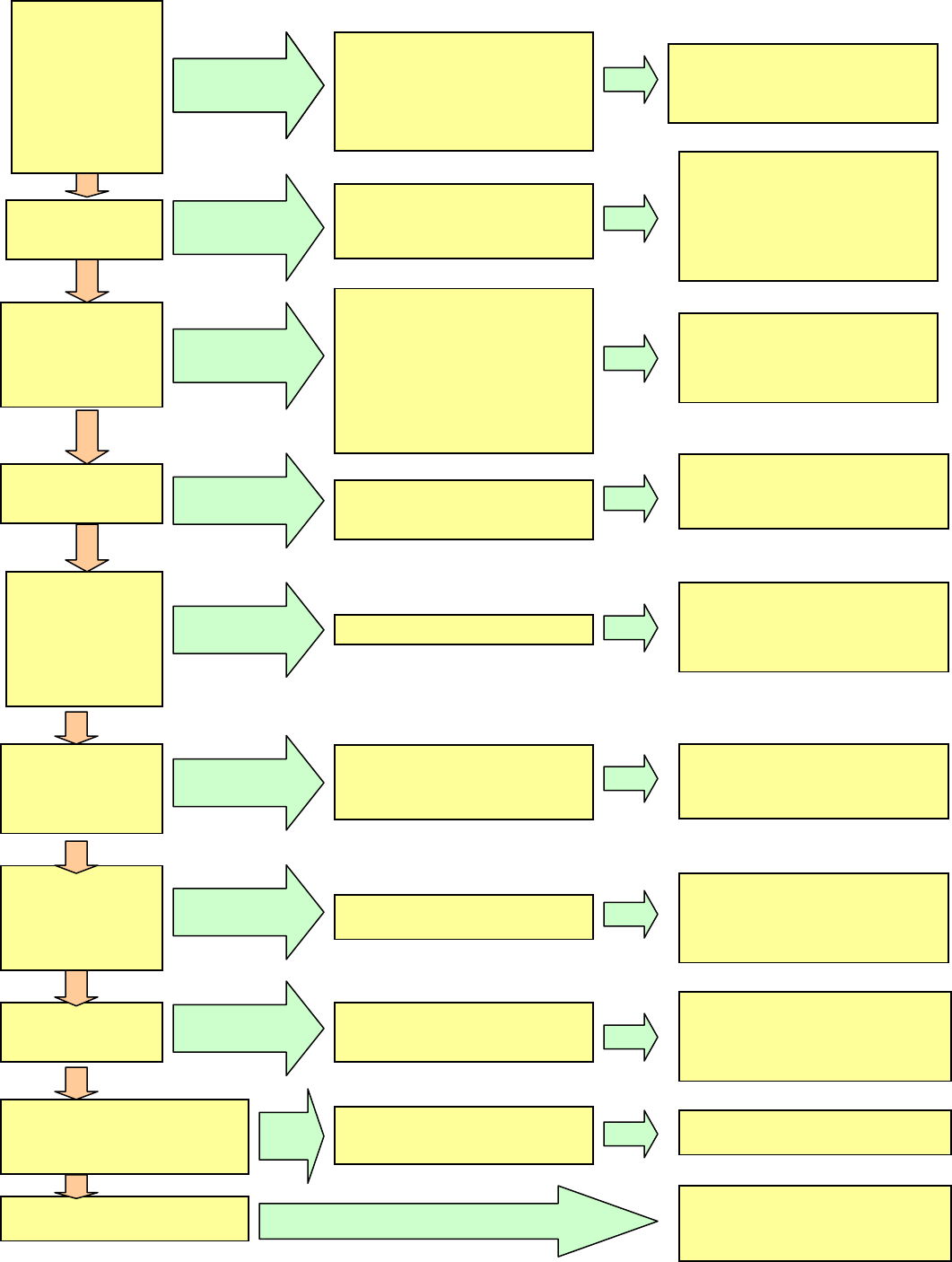
Anxiety
Consider the role of a
general medical
conditio n
(Hyperthyroidism,
Respiratory Illness,
Cardiac disease) or
substance use and
whether the anxiety is
better accounted for
by another mental
disorder.
A) Anxiety disorder due to a general
medical condition
B) Alcohol-induced anxiety disorder or
Substance-induced anxiety disorder.
C) Other Mental Disorder
-Complete Medical Work-up or
Substance Treatment Referral to
RBHA clinic
Do the presenting
symptoms include one
or more panic attacks?
Do the presenting
symptoms include fear
of separation?
Do the presenting
symptoms include fear,
avoidance or anxious
anticipation about one
or more specific
situations?
Are the presenting
anxiety symptoms
related to re-
experiencing highly
traumatic events?
Is the presenting worry
or anxiety related to
recurrent or persistent
thoughts (obsessions)
and/or ritualistic
behaviors or recurrent
mental acts
(compulsion)?
Have pervasive anxiety
symptoms and worry
been associated with a
variety of events or
situations and persisted
more than 6 months.
Are the symptoms in
response to a specific,
psychosocial stressor?
Is the anxiety clinically significant and
are criteria not met for any of the
previously described specific
disorders?
Reconsider medical condition or
substance abuse
A) Panic disorder without
agoraphobia
B) Panic attacks occurring within the
context of an anxiety disorder
A) Social phobia (avoidance of social
situations)
B) Specific phobia (avoidance of a specific
object or situation)
C) Panic disorder w/agoraphobia (avoidance
of situations in which escape may be
difficult in the event of panic)
D) Agoraphobia without history of panic
disorder (avoidance of a situation in which
escape may be difficult)
Separation anxiety disord er (anx iety
concerning separation from a major
attachment)
A) PSTD (of symptoms persist at
leas t 4 weeks)
B) Acute Stress Disorder (if symptoms
persist for less than 4 weeks)
Generalized Anxiety Disorder
Adjustment disorder with anxiety or
Adjustment disorder with mixed anxiety
and depressed mood
Anxiety disorder, N.O.S.
Adjustment disorder with mixed anxiety
and depressed mood
-Consider referral for psychotherapy to
RBHA clinic
-Consider SSRI and/or office based
anxiolytic therapy or re-evaluate wellness
once a week
-Consider psychiatric telephonic
consultation with RBHA psychiatrics or
case transfer
-Consider psychotherapy referral to
RBHA clinic
-Consider telephonic consultation with
RBHA psychiatrist and office based
medication management or case transfer
Obsessive-compulsive disorder
-Consider psychotherapy referral to the
RBHA clinic
-Consider telephonic consultation with
RBHA Psychiatrist or case transfer
-Consider short-term medical management
and referral to RBHA clinic
-Medical and psychiatric differential
diagnostic assessment required
-Medical e valuati on is nega tive, refer to
RBHA clinic
-Consider psychotherapy referral to the
RBHA clinic and office based medication
management
-Consider telephone consultation with
RBHA Psychiatrist or case transfer
-Consider psychotherapy referral or RBHA
clinic and medication management
-Consider telephone consultation with
RBHA Psychiatrist or case transfer
-Consider psychotherapy referral or
reassessment within a week and/or office
based medication management
-Consider telephonic consultation with
RBHA Psychiatrist or case transfer
-Consider psychotherapy referral to RBHA
clinic and office based medication
management
-Consider telephonic consultation with
RBHA Psychiatrist or case transfer
YES
Expand clinical questioning
yes
yes
yes
yes
yes
yes
yes
yes
yes
*Based on algorithms developed g uide to P sychiatric diagnosis in primary care
*Sole usage of Algorithms is not a substitute for a comprehensive clinical assessment
Pingitore, D and Sansone, R., American Family Physicians, Vol. 58/no.6 (1998)
YES
Expand clinical questioning
YES
YES
YES
Expand clinical questioning
YES
Expand clinical questioning
YES
Expand clinical questioning
YES
Expand clinical questioning
YES
Expand clinical questioning
YES
Expand clinical questioning
YES
Expand clinical questioning
no
no
no
no
no
no
no
no
no
Diagnoses are defined in DMS-IV-TR

How much stress or worry is considered too much? Complete the following self-test by clicking the "yes" or
"no" boxes next to each question, print out the page, and show the results to your health care professional.
IS IT AN ANXIETY DISORDER?
Yes or No? As a teenager are you troubled by
More days than not, do you:
More days than not, do you feel:
Reference
Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. Washington, DC, American Psychiatric
Association, 1994.
ANXIETY DISORDERS IN ADOLESCENTS: A SELF-TEST
Yes No
Repeated, unexpected "attacks" during which you suddenly are
overcome by intense fear or discomfort for no apparent reason, or the
fear of having another panic attack?
Yes No
Persistent, inappropriate thoughts, impulses or images that you can't
get out of your mind (such as a preoccupation with getting dirty or worry
about the order of things)?
Yes No
Distinct and ongoing fear of social situations involving unfamiliar
people?
Yes No
Excessive worrying about a number of events or activities?
Yes No
Fear of places or situations where getting help or escape might be
difficult, such as in a crowd or on an elevator?
Yes No
Shortness of breath or racing heart for no apparent reason?
Yes No
Persistent and unreasonable fear of an object or situation, such as
flying, heights, animals, blood, etc.?
Yes No
Being unable to travel alone, without a companion?
Yes No
Spending too much time each day doing things over and over again (for
example, hand washing, checking things, or counting)?
Yes No
Feel restless?
Yes No
Feel easily fatigued or distracted?
Yes No
Experience muscle tension or problems sleeping?
Yes No
Sad or depressed?
Yes No
Disinterested in life?
Yes No
Worthless or guilty?
Yes No
Have you experienced changes in sleeping or eating habits?
Yes No
Do you relive a traumatic event through thoughts, games, distressing
dreams, or flashbacks?
Yes No
Does your anxiety interfere with your daily life?
Reference
Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. Washington, DC, American Psychiatric
Association, 1994.
ANXIETY DISORDES IN CHILDREN: A TEST FOR PARENTS
If you think your child may have an anxiety disorder, please answer the following questions
"Yes" or "No", print out the page, and show the results to your child's health care professional:
Yes No
Does the child have a distinct and ongoing fear of social situations
involving unfamiliar people?
Yes No
Does the child worry excessively about a number of events or
activities?
Yes No
Does the child experience shortness of breath or a racing heart for no
apparent reason?
Yes No
Does the child experience age-appropriate social relationships with
family members and other familiar people?
Yes No
Does the child often appear anxious when interacting with her peers
and avoid them?
Yes No
Does the child have a persistent and unreasonable fear of an object or
situation, such as flying, heights, or animals?
Yes No
When the child encounters the feared object or situation, does he react
by freezing, clinging, or having a tantrum?
Yes No
Does the child worry excessively about her competence and quality of
performance?
Yes No
Does the child cry, have tantrums, or refuse to leave a family member
or other familiar person when she must?
Yes No
Has the child experienced a decline in classroom performance, refused
to go to school, or avoided age-appropriate social activities?
Yes No
Does the child spend too much time each day doing things over and
over again (for example, hand washing, checking things, or counting)?
Yes No
Does the child have exaggerated fears of people or events (i.e.,
burglars, kidnappers, car accidents) that might be difficult, such as in a
crowd or on an elevator?
Yes No
Does the child experience a high number of nightmares, headaches, or
stomachaches?
Yes No
Does the child repetitively re-enact with toys scenes from a disturbing
event?
Yes No
Does the child redo tasks because of excessive dissatisfaction with
less-than-perfect performance?

ANXIETY
UNIVERSALLY AVAILABLE MEDICATIONS THROUGH
AHCCCS HEALTH PLANS AND RBHA PROVIDER*
SELECTIVE SEROTONIN REUPTAKE
INHIBITOR
Fluoxtetine (Prozac)
Paroxetine (Paxil)
Sertraline (Zoloft)
TRICYCLIC ANTIDEPRESSANT
Imipramine (Tofranil)
BENZODIAZEPINE
Lorazepam (Ativan)
Clonazepam (Klonopin)
SEROTONIN PARTIAL AGONIST
Buspirone (Buspar)
*Refer to health plan for prior authorization requirements and medication availability.
Initial Effective Date: 05/01/2009 Revision Date: 05/01/2011


