
Fillable Printable Application For An American Legion License Plate
Fillable Printable Application For An American Legion License Plate
Application For An American Legion License Plate
MVR-27AL
(Revised 9/2017)
North Carolina Division of Mot or Ve
hicles
3155 Mail Service Center
Raleigh, NC 27697-3155
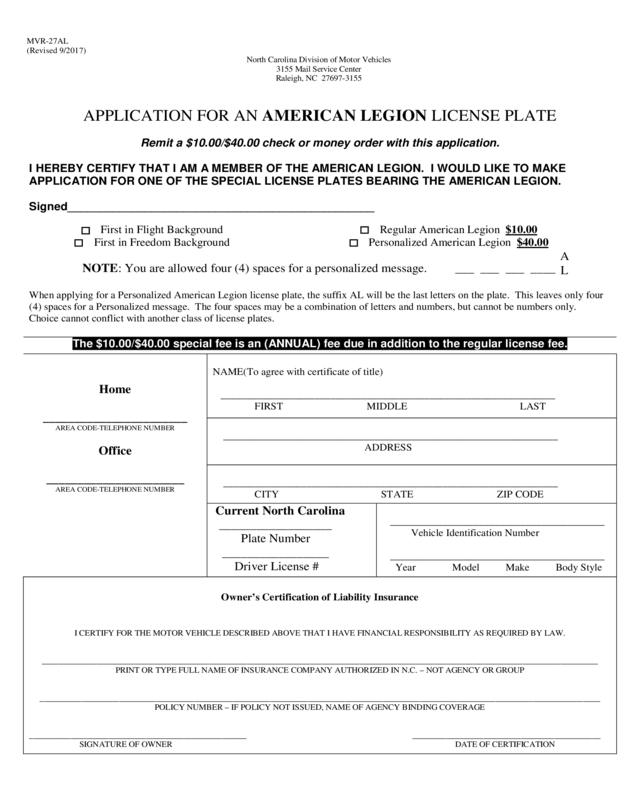
APPLICATION FOR AN AMERICAN LEGION LICENSE PLATE
Remit a $10.00/$40.00 check or money order with this application.
I HEREBY CE
RTIFY THAT I AM A MEMBER OF THE AMERICAN LEGION. I WOULD LIKE TO M AKE
APPLICATION FO R ONE OF THE SPECI AL LICENSE PLATES BEARING THE AMERICAN LEGION.
Signed________________________________________________
First in Flight Background
First in Freedom Background
Regular American Legion $10.00
Personalized American Legion $40.00
NOTE: You are allowed four (4) spaces for a personalized message. ___ ___ ___ ____
A
L
When applying for a Personalized American Legion license plate, the su f fi x A L will be the last letters on the plate . T his leaves only fo ur
(4) spaces for a Personalized message. The four spaces may be a combination of letters and numbers, but cannot be numbers only.
Choice cannot conflict with a nother class of license plates.
The $10.00/$40.00 special fee is an (ANNUAL) fee due in addition to the regular license fee.
Home
_______________________
AR EA CODE-TE LE PHON E N U MBER
Office
______________________
AR EA CODE-TE LE PHON E N U MBER
NAME(To agree with certificate of title)
____________
____________________________________________________
FIRST MIDDLE LAST
________________________________________________________________
ADDRESS
________________________________________________________________
CITY STATE ZIP CODE
Current North Carolina
__________________
Plate Number
_________________
Driver License #
_________________________________________
Vehicle Identifica tion Number
____________
_____________________________
Year Model Make Body Style
Owner’s Certif ic ation of Liability Insur ance
I CERTIFY FOR THE M OTOR VEHICLE DESCRIBED ABOVE THAT I HAVE FINANCIAL RESPONSIBILITY AS RE QUIRED BY LAW.
______
_______________________________________________________________________________________________________________________________
PRINT OR TYPE FULL NAME OF INSURANCE COM PANY AUTHOR IZED IN N.C. – NOT AGENCY OR GROUP
______
________________________________________________________________________________________________________________________________
POLICY NUMBE R – IF POLICY NOT ISSUED, NAME OF AGENCY BINDING COVERAGE
______
_____________ ________________________ _________ _____________________________________________
SIGNATURE OF OWNER DATE OF CERTIFICATION


