
Fillable Printable Application For Elective Coverage Of Sdi Only Local Public Entities And Indian Tribes (De 1378M)
Fillable Printable Application For Elective Coverage Of Sdi Only Local Public Entities And Indian Tribes (De 1378M)
Application For Elective Coverage Of Sdi Only Local Public Entities And Indian Tribes (De 1378M)
DE 1378M Rev. 11 (8-16) (INTERNET) Page 1 of 2 CU
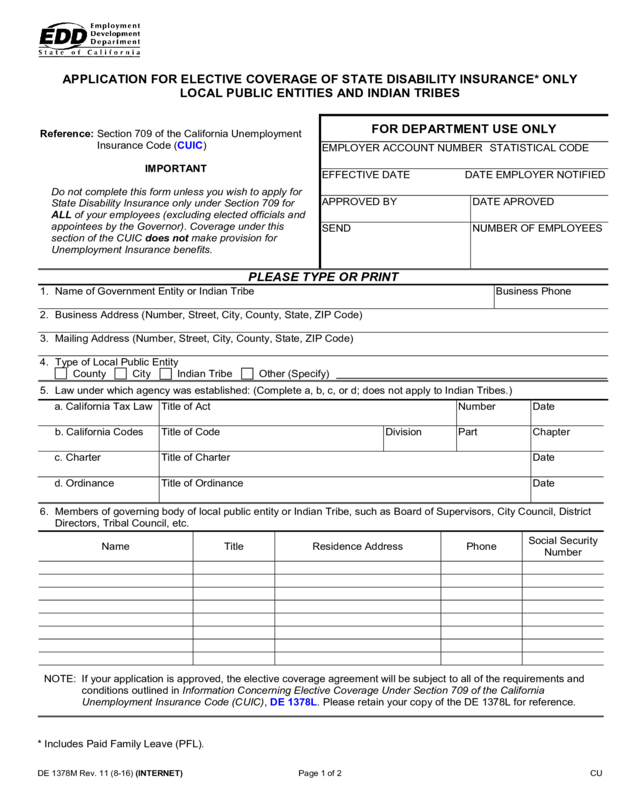
APPLICATION FOR ELECTIVE COVERAGE OF STATE DISABILITY INSURANCE* ONLY
LOCAL PUBLIC ENTITIES AND INDIAN TRIBES
Reference: Section 709 of the California Unemployment
Insurance Code (CUIC)
I
MPORTANT
D
o not complete this form unless you wish to apply for
State Disability Insurance only under Section 709 for
ALL of your employees (excluding elected officials and
appointees by the Governor). Coverage under this
section of the CUIC does not make provision for
Unemployment Insurance benefits.
FOR DEPARTMENT USE ONLY
EMPLOYER ACCOUNT NUMBER STATISTICAL CODE
EFFECTIVE DATE DATE EMPLOYER NOTIFIED
APPROVED BY
DATE APROVED
SEND
NUMBER OF EMPLOYEES
PLEASE TYPE OR PRINT
1. Name of Government Entity or Indian Tribe
Business Phone
2. Business Address (Number, Street, City, County, State, ZIP Code)
3. Mailing Address (Number, Street, City, County, State, ZIP Code)
4. Type of Local Public Entity
County City Indian Tribe Other (Specify)
5. Law under which agency was established: (Complete a, b, c, or d; does not apply to Indian Tribes.)
a. California Tax Law
Title of Act
Number
Date
b. California Codes
Title of Code
Division
Part
Chapter
c. Charter
Title of Charter
Date
d. Ordinance
Title of Ordinance
Date
6. Members of governing body of local public entity or Indian Tribe, such as Board of Supervisors, City Council, District
Directors, Tribal Council, etc.
Name Title Residence Address Phone
Social Security
Number
NOTE: If your application is approved, the elective coverage agreement will be subject to all of the requirements and
conditions outlined in Information Concerning Elective Coverage Under Section 709 of the California
Unemployment Insurance Code (CUIC), DE 1378L. Please retain your copy of the DE 1378L for reference.
* Includes Paid Family Leave (PFL).
DE 1378M Rev. 11 (8-16) (INTERNET) Page 2 of 2 CU
7. Appointive Positions: (These persons are eligible for coverage unless appointed by the Governor.)
Title of Position
Number of
Positions in This
Category
By Whom Appointed
Number of
Persons Desiring
Coverage
8. Total number of employees to be covered, excluding elected officers and those appointed by the Governor:
9. On what date do you wish elective coverage to commence? Keep in mind that the commencement date of an elective
coverage agreement shall not be prior to the first day of the calendar quarter in which the application is filed, nor later
than the first day of the following calendar quarter.
First day of current quarter First day of next quarter
NOTE: Deductions should not be made from your employee's wages for the purpose of paying employee contributions
required under the CUIC until your election is approved.
Attach a copy of the resolution in which the governing body described in Item 6 approved the filing of an application for
elective coverage under Section 709 of the CUIC.
The governmental or tribal entity described in Item 1 hereby files its application under Section 709 of the CUIC to become
an employer subject to the CUIC. It is understood that upon approval of the election by the Director, the governmental or
tribal entity will be an employer subject to the CUIC for State Disability Insurance purposes only to the same extent as
other employers as of the date specified in the approval, and will remain a subject employer for at least two complete
calendar years. Thereafter, this election may be terminated as provided by the CUIC.
I certify that this application has been examined by me, and to the best of my knowledge and belief, it is true and correct
and made in good faith under the provisions of the CUIC.
This certificate must be signed by one or more of the persons listed under Item 6.
Signature Title Date
Return completed application to:
Employment Development Department
Analysis Resolution and Correspondence Organization
PO Box 2068
Rancho Cordova, CA 95741-2068
Questions may be directed to the above address or call 888-745-3886.
The EDD is an equal opportunity employer/program. Auxiliary aids and services are available upon request to individuals
with disabilities. Requests for services, aids, and/or alternate formats need to be made by calling 888-745-3886 (voice) or
TTY 800-547-9565.


