
Fillable Printable Application For Supplemental Income Benefits
Fillable Printable Application For Supplemental Income Benefits
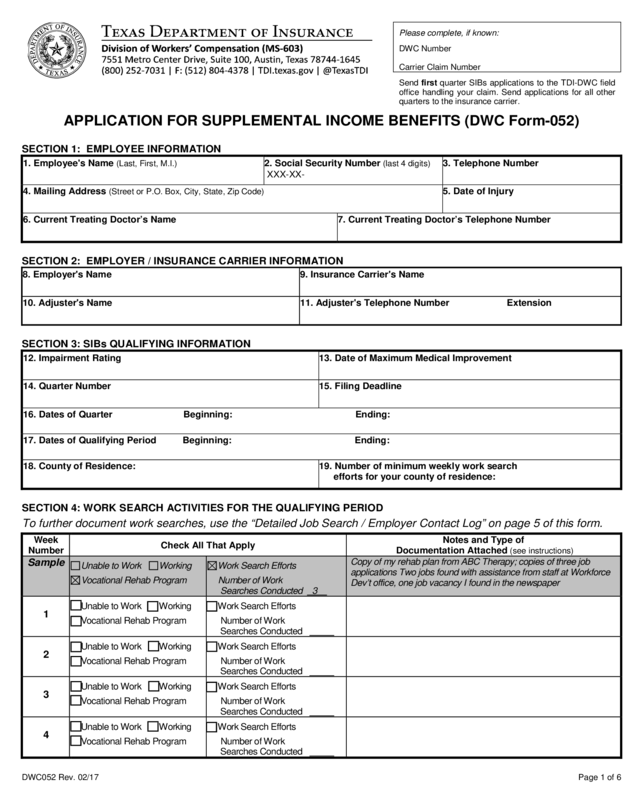
Application For Supplemental Income Benefits
DWC052 Rev. 02/17 Page 1 of 6
P
lease complete, if known:
DWC Numbe r
Carrier Claim Number
Send first quarter SIB s applications to t he TDI-DW C field
office handling your claim. Send applications for all other
quarters to the insurance carrier.
APPLICATION FOR SUPPLEM E NTAL INCOME BENEFITS (DWC Form-052)
SEC
TION 1: EMPLOYEE INFORMATION
1. Employee's Name
(Last, Fir st , M .I.)
2. Social Security Number
(last 4 digits )
XXX-XX-
3. Telephone Number
4. Mailing Address
(Street or P.O. Box, City, State, Zip Code)
5. Date of Injury
6. Current Treating Doctor’s Name
7. Current Treating Doctor’s Telephone Number
SECTION 2: EMPLOYER / INSURANCE CARRIER INFORMATION
8. Employer's Name
9. Insurance Carrier's Name
10. Adjuster's Name
11. Adjuster's Telephone Number Extension
SECTION 3: SIBs QUALIFYING INFORMATION
12. Impairment Rating
13. Date of Maximum Medical Improvement
14. Quarter Number
15. Filing Deadline
16. Dates of Quarter Beginning: Ending:
17. Dates of Qualifying Period Beginning: Ending:
18. County of Residence:
19. Number of minimum weekly work search
efforts for your county of residence:
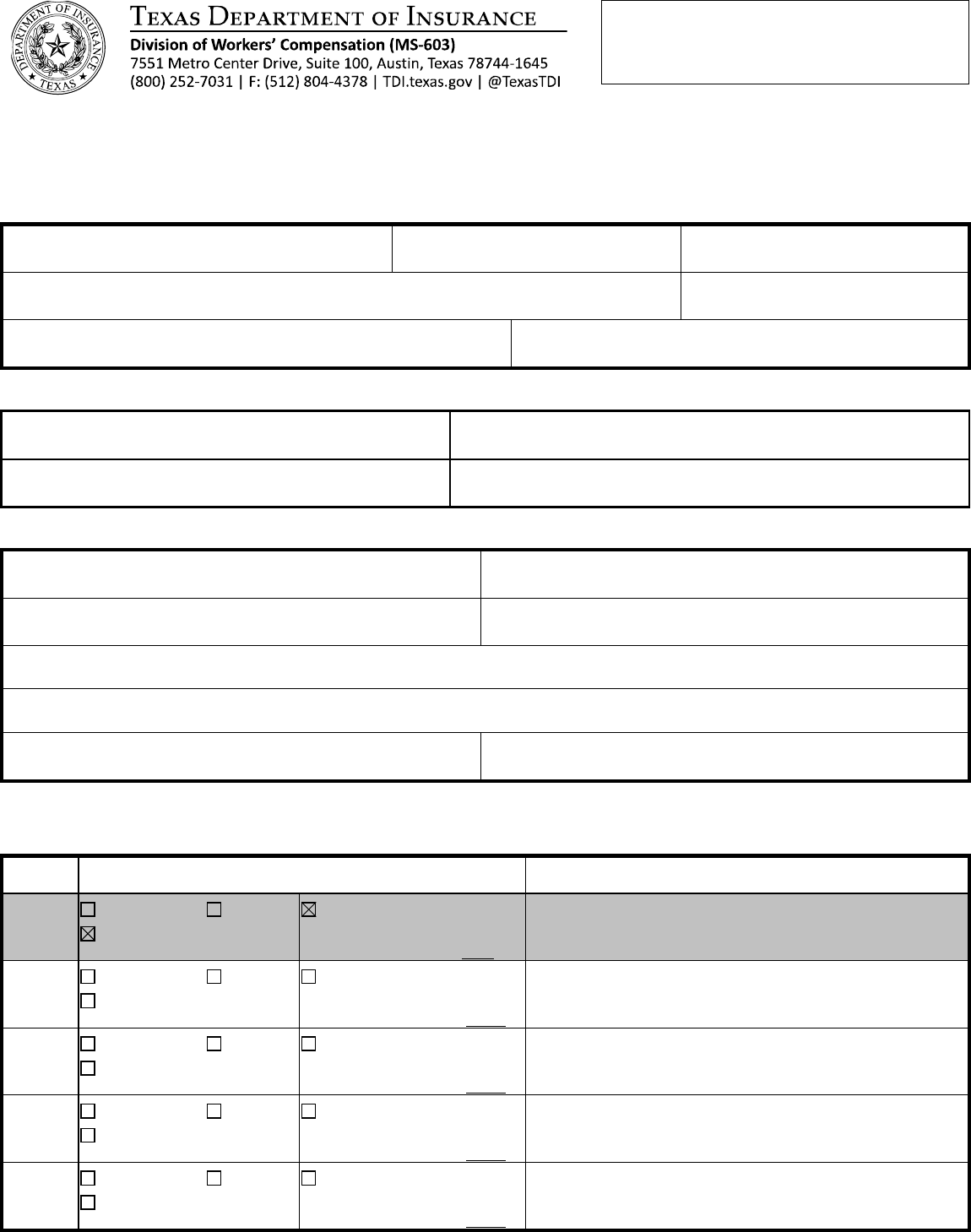
SECTION 4: WORK SEARCH ACTIVITIES FOR THE QUALIFYING PERIOD
To further document work searches, use the “Detailed Job Search / Employer Contact Log” on page 5 of th is form .
Week
Number
Check All That Apply
Notes and Type of
Documentation Attached (see instructions)
Sample
Unable to Work Working
Vocational Rehab Program
Work Search Efforts
Num ber of Wor k
Searches Conducted 3
Copy of my rehab plan from ABC Therapy; copies of three job
applications Two jobs found with assistance from staff at Workforce
Dev’t office, one job vacancy I found in the newspaper
1
Unable to Work Working
Vocational Rehab Program
Work Search Efforts
Number of Work
Searches Conducted
2
Unable to Work Working
Vocational Rehab Program
Work Search Efforts
Number of Work
Searches Conducted
3
Unable to Work Working
Vocational Rehab Program
Work Search Efforts
Number of Work
Searches Conducted
4
Unable to Work Working
Vocational Rehab Program
Work Search Efforts
Number of Work
Searches Conducted
DWC052 Rev. 02/17 Page 2 of 6
Week
Number
Check All That Apply
Notes and Type of
Documentation Attached (see instructions)
5
Unable to Work Working
Vocational Rehab Program
Work Search Efforts
Number of Work
Searches Conducted
6
Unable to Work Working
Vocational Rehab Program
Work Search Efforts
Number of Work
Searches Conducted
7
Unable to Work Working
Vocational Rehab Program
Work Search Efforts
Number of Work
Searches Conducted
8
Unable to Work Working
Vocational Rehab Program
Work Search Efforts
Number of Work
Searches Conducted
9
Unable to Work Working
Vocational Rehab Program
Work Search Efforts
Number of Work
Searches Conducted
10
Unable to Work Working
Vocational Rehab Program
Work Search Efforts
Number of Work
Searches Conducted
11
Unable to Work Working
Vocational Rehab Program
Work Search Efforts
Number of Work
Searches Conducted
12
Unable to Work Working
Vocational Rehab Program
Work Search Efforts
Number of Work
Searches Conducted
13
Unable to Work Working
Vocational Rehab Program
Work Search Efforts
Number of Work
Searches Conducted
SECTION 5: WAGES DURING QUALIFYING PERIOD
Week Ending
Gross Wages Earned
Week Ending
Gross Wages Earned
1. $ 8. $
2. $ 9. $
3. $ 10. $
4. $ 11. $
5. $ 12. $
6. $ 13. $
7.
$
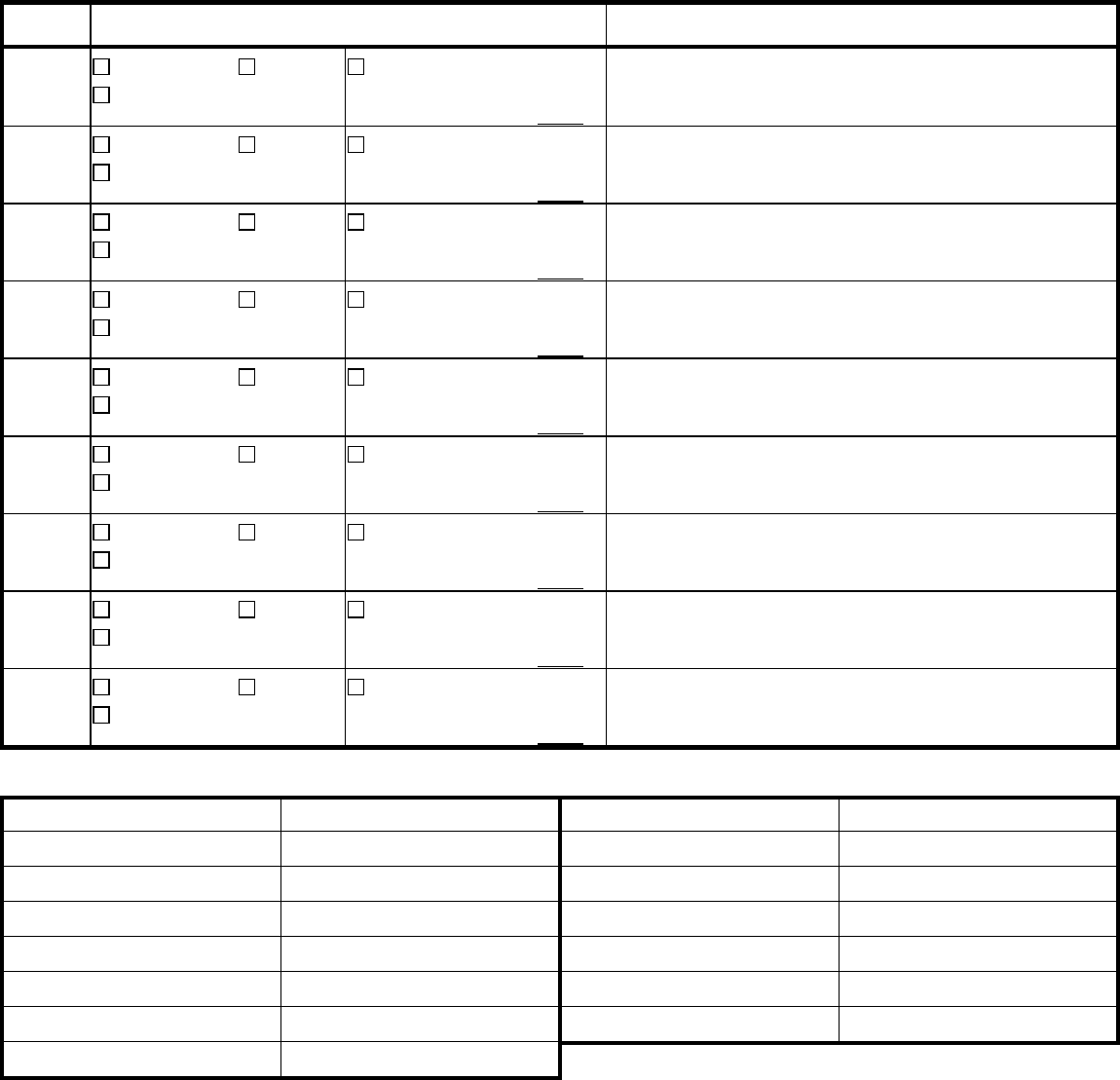
SECTION 6: CERTIFICATION
I certify that:
• I have not elected to have any of my impairment income benefits paid in a lump sum;
• I am earning less than 80% of my average weekly wage as a result of my impairment from my compensable injury;
• I have complied with the Texas Department of Insurance, Division of Workers’ Compensation (TDI-DWC) Work Searc
h
R
equirements (Texas Labor Code § 408.1415 and Texas Administrative Code §130.101 and §130.102); and,
• the information I have provided on this Application for Supplemental Income Benefits is true. I understand that if I
intentionally provide false information to obtain benefits, I can be charged with an administrative or criminal penalty.
E
mployee’s Signature ___________________________________________ Date ________________
DWC052 Rev. 02/17 Page 3 of 6
SECTION 7: NOTICE OF ENTITLEMENT OR NON-ENTITLEMENT
Quarter Num ber
Beginning Date
Ending Date
TO BE C OMPLETED BY TDI-DWC FOR FIRST QUARTER
AND B Y INSURA NCE CA RRIER FOR SU BSEQ UENT QUA RT ERS.
Employee Entitled to Supplemental Income Benefits Monthly Payments for 3 Months $
Employee No t Entitled to Supplementa l Income Benefits
Reason for Non-entitlement:
Signature of Reviewing Authority
Date
Printed Name of Reviewing Authority
Title
Telephone Number
INFORMATION FOR DISPUTING ENTITLEMENT OR AMOUNT OF SUPPLEMENTAL INCOME BENEFITS:
To Employee
• To dispute non-entitlement to supplemental income benefits or the monthly amount to be paid in any quarter, you must have facts, such as
your detailed job search/employ er contact log or a current narrative report from your doctor supporting your disability, or a legal basis.
• To dispute the determination by TDI-DWC or the insurance carrier, you must request a benefit review conference by contacting the TDI-DWC
office handling your claim or call (800) 252-7031.
To Insurance Carrier
• To dispute the first quarter, request a benefit review conference within 10 days after receiving notice from TDI-DWC.
• To dispute entitlement to a subsequent quarter when payment has been made in the previous quarter, request a benefit review conference
within 10 days after receiving the employee's Application for Suppleme ntal Inc om e Ben efit s .
• To dispute entitlement to a subsequent quarter without prior payment in the previous quarter, send the notice of non-entitlement to the
employee within 10 days of the date the form was filed with the insurance carrier. Include the reason(s) for finding non-entitlement and give
instructions to the employee about how to dispute the insurance carrier's determination.
CALCUL ATION OF SUPPLEMENT AL INCOME BENEFITS
To Be Completed By TDI-DWC Or Insurance Carrier To Show Wages Used To Calculate Monthly Payments
1.
$
x
80%
=
$
(Average Weekly Wage)
(Transfer to Line 4A)
2.
$
+
$
=
$
(Earned Wages)
(Offered Wages)
(Transfer to Line 3A)
3.
$
÷
13
=
$
(3A - Total Wages)
(Transfer to Line 4B)
4.
$
$
=
$
(4A)
(4B)
(Transfer to Line 5A)
5.
$
x
80%
=
$
(5A)
(Transfer to Line 6A)
6.
$
x
4.34821
=
$
(6A)
(Monthly Payment*)
If Contribution: (% )
7.
$
x
=
$
(Monthly Payment)
(% of Reduction)
(Transfer t o Line 8B)
8.
$
$
=
$
(Monthly Payment)
(8B - Contribution Reduction)
(Reduced Monthly Payment)
*
Subject to a maximum amount.
DWC052 Rev. 02/17 Page 4 of 6
APPLICATION FOR SUPPLEMENTAL INCOME BENEFITS (DWC Form-052)
To complete this application, refer to the TDI-DWC publication
“Questions and Answers about Supplem ental Income Benefits.”
When do I file th e application for SIBs?
The SIBs application deadlines will be different for each injured employee, depending on the dates of the qualifying period.
Generally, you must submit your application for SIBs six days before the end of the qualifying period, but no later than seven
days af ter the e nd date of the q ualif ying per iod. For t h e firs t quarter, t his f iling de adline is pro vide d for you in Item #4 of the SIBs
notification letter sent to you by the Texas Department of Insurance, Division of Workers’ Compensation (TDI-DWC). For other
quarters, your insur a nce ca r rier will provid e you with the filing deadline in Section 3, Item # 15 of this form.
Where do I send the completed form?
For the first quarter, send the completed DW C Form-052 and supporting documentation to the TDI-DWC Field Office handling
your claim. Field office contact information is available at http://www.tdi.texas.gov/wc/dwccontacts.html#offices
. For all other
quarters, return the form to your insurance carrier. You may file the form by first class mail, personal delivery or electronic
submission (including fax or e-mail).
How many job applications and/or work search contacts must I make if I am actively seeking work?
You must make at least the minimum number of job applications and/or work search contacts consistent with those for
unemplo ymen t compensati on benefits. T hese vary b y count y of r esidence. You must contact TDI-DWC at 1-800-252-7031 or g o
to the website at http://www.tdi.texas.gov/wc/employee/suppben.html
to find the number of minimum weekly work search
requirements for the county where you live.
What documentation should I provide to show that I meet TDI-DWC’s work search requirements?
You must maintain supporting documentation, applications, letters, and notes to clearly demonstrate your active efforts to meet
the TDI-DWC work search requirements for each week during the entire qualifying period. The following are examples of the
various types of acceptable documentation.
To Document Work Searches - If you have not returned to work and you are able to work in any capacity, you must look for a job
to match your ability to work during each week of the qualifying period. Appropriate documentation includes:
• Work search log attached to DWC Form-052, Application for Supplemental Income Benefits;
• Documentation about any follow-up visits to a potential employer; and/or
• Copies of employment applications or resumes which document your efforts to find a job.
If you have any of fers of em ployment which you do not accept, you m ust includ e infor mation about the offered wa ges as part of
this application. If you are self-employed, show your gross weekly wages as the total amount of income received from self-
employment. Use the attached “Detailed Job Search / Employer Contact Log” (page 5 of this form) to document your efforts.
To Document an Inability to Work - If you are unable to work due to your com pensable injury for any part or all of the qualifying
period, you must submit a narrative report from a doctor which specifically explains how your compensable injury caused your
inability to perform any kind of work for the specific period of time.
To Document Participation in Vocational Rehabilitation Services - If you participate in a Vocational Rehabilitation Services
program, you must provide documentation to show your efforts to meet the requirements of your vocational rehabilitation plan.
To Document Employment During the SIBs Qualifying Period - You must provide documentation that you earned less than 80%
of your average weekly wage as a direct result of your impairment from the compensable injury. Appropriate documentation
includes payroll stubs and wage statements.
When and how will I know if I a m approved for SIBs?
TDI-DWC will notify you of fir st quar ter SI Bs entit lement no later th an the last day of your IIBs perio d. For all s ubs equ ent q uarters,
the insuranc e carr ier mus t notify app licants of its deci sion of SI Bs entitl ement wit hin 10 da ys of the receipt o f an applica tion. T he
notice will contain specific information regarding the reason for its determination. If you are denied SIBs, the notice will include the
grounds for the determination, the beginning and ending dates of the quarter, and instructions for the parties if they want to
dispute the decision.
Where do I find more information regarding SIBs?
More information about SIBs, including a listing of each Texas county’s number of minimum work searches and the TDI-DWC
publication “Questions and Answers about Supplemental Income Benefits,” is available on the website at
http://www.tdi.texas.gov/wc/employee/suppben.html
.
NOTE: With few exceptions, upon your request, you are entitled to be informed about the information TDI-DWC collects about you; get and
review the information (Government Code, §§552.021 and 552.023); and have TDI-DWC correct information that is incorrect (Government
Code, §559.004). For more information, contact agencycounsel@tdi.texas.gov or you may refer to the Corrections Procedure
section at
www.tdi.texas.gov.
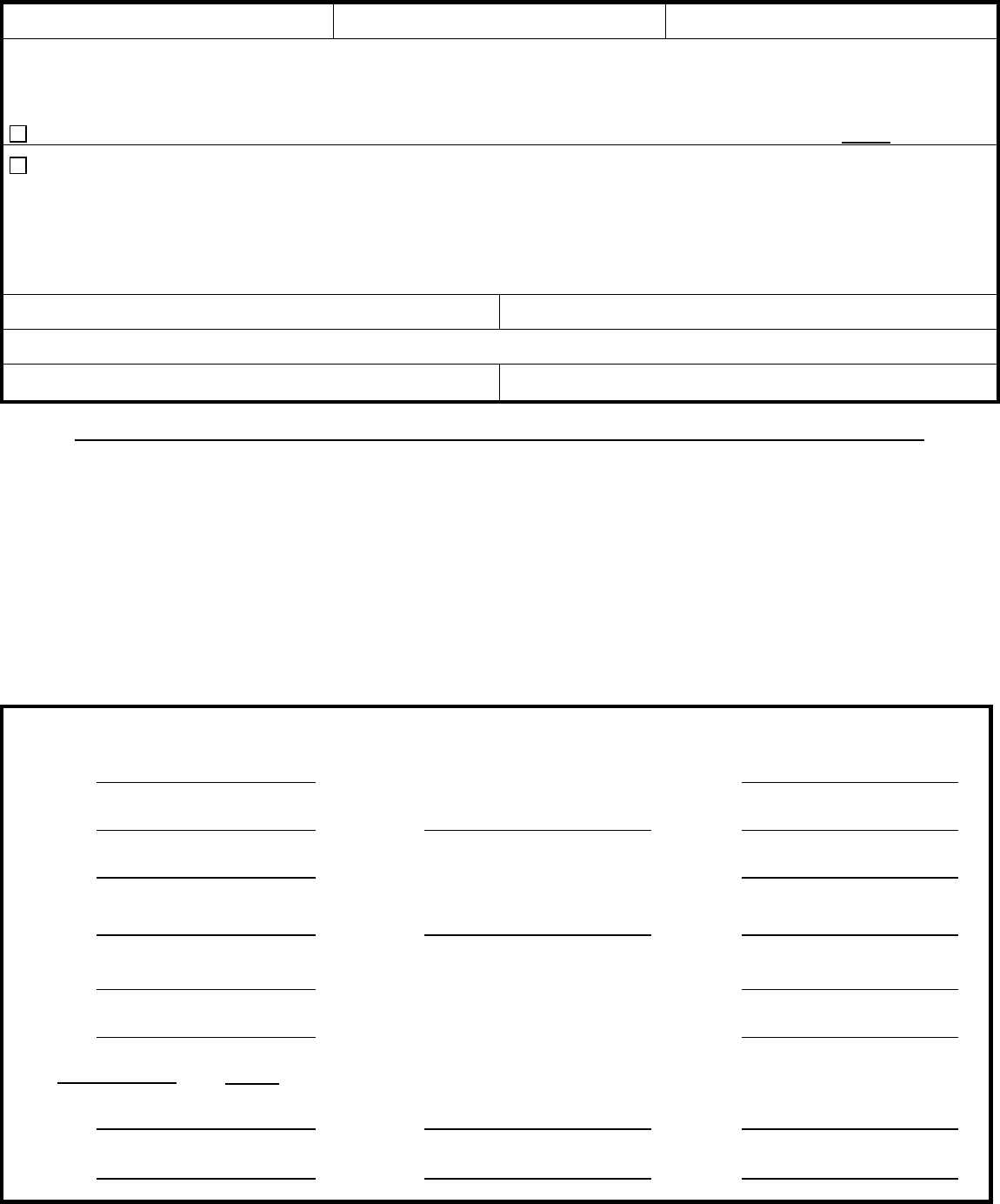
DWC052 Rev. 02/17 Page 5 of 6
Detailed Job Search / Employer Contact Log (provide detail for each job contact)
Name: Number of minimum weekly work search efforts for your county of residence:
Date
(mm/dd/yyyy)
Business Na
me, Address,
Phone and Website
Contacted Submitted Person Contacted Description
of Job
Results
In person
By phone
By fax
By mail
By e-mail /
web
Cover letter
Application
Resume
Name
Phone
Fax
E-mail
Job offered
Amount of
wages offered
Accepted offer?
Yes No
Start date
Not hiring
Other
In person
By phone
By fax
By mail
By e-mail /
web
Cover letter
Application
Resume
Name
Phone
Fax
E-mail
Job offered
Amount of
wages offered
Accepted offer?
Yes No
Start date
Not hiring
Other
In person
By phone
By fax
By mail
By e-mail /
web
Cover letter
Application
Resume
Name
Phone
Fax
E-mail
Job offered
Amount of
wages offered
Accepted offer?
Yes No
Start date
Not hiring
Other
In person
By phone
By fax
By mail
By e-mail /
web
Cover letter
Application
Resume
Name
Phone
Fax
E-mail
Job offered
Amount of
wages offered
Accepted offer?
Yes No
Start date
Not hiring
Other
INJURED EMPLOYEES MUST DOCUMENT EACH EMPLOYER CONTACT- USE ADDITIONAL PAGES AS NEEDED
DWC052 Rev. 02/17 Page 6 of 6
Detailed Job Search / Employer Contact Log (provide detail for each job contact)
Name: Number of minimum weekly work search efforts for your county of residence:
Date
(mm/dd/yyyy)
Business Na
me, Address,
Phone and Website
Contacted Submitted Person Contacted Description
of Job
Results
In person
By phone
By fax
By mail
By e-mail /
web
Cover letter
Application
Resume
Name
Phone
Fax
E-mail
Job offered
Amount of
wages offered
Accepted offer?
Yes No
Start date
Not hiring
Other
In person
By phone
By fax
By mail
By e-mail /
web
Cover letter
Application
Resume
Name
Phone
Fax
E-mail
Job offered
Amount of
wages offered
Accepted offer?
Yes No
Start date
Not hiring
Other
In person
By phone
By fax
By mail
By e-mail /
web
Cover letter
Application
Resume
Name
Phone
Fax
E-mail
Job offered
Amount of
wages offered
Accepted offer?
Yes No
Start date
Not hiring
Other
In person
By phone
By fax
By mail
By e-mail /
web
Cover letter
Application
Resume
Name
Phone
Fax
E-mail
Job offered
Amount of
wages offered
Accepted offer?
Yes No
Start date
Not hiring
Other
INJURED EMPLOYEES MUST DOCUMENT EACH EMPLOYER CONTACT- USE ADDITIONAL PAGES AS NEEDED


