
Fillable Printable Blank Commercial Driver Application
Fillable Printable Blank Commercial Driver Application
Blank Commercial Driver Application
1
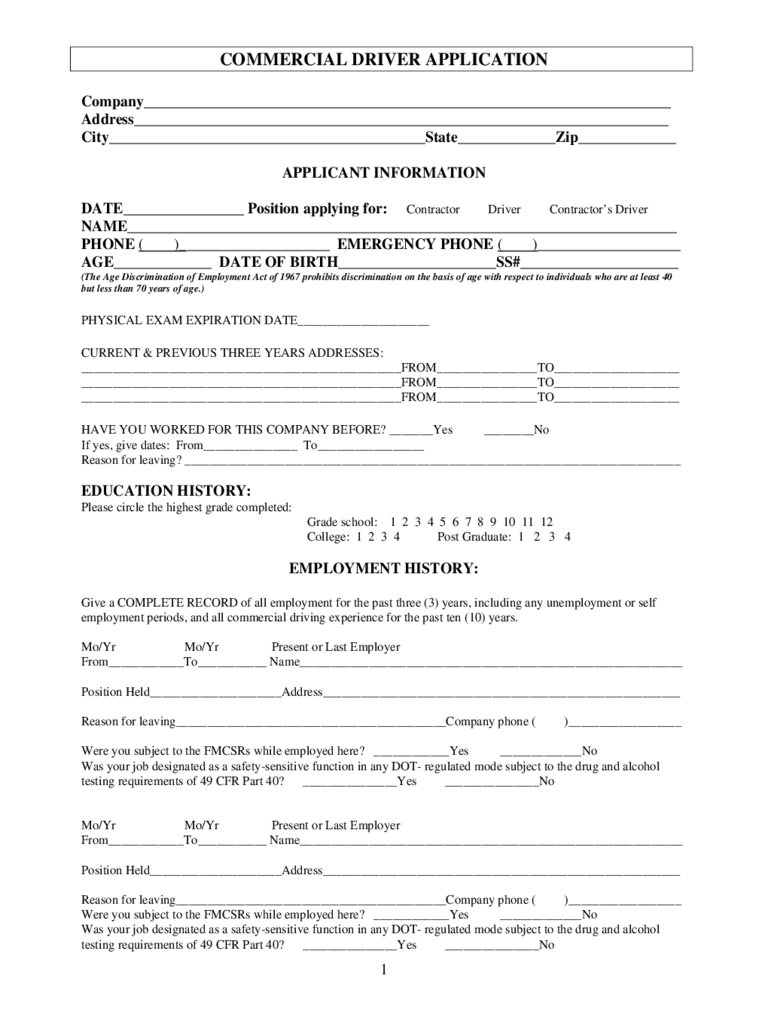
COMMERCIAL DRIVER APPLICATION
Company______________________________________________________________________
Address_______________________________________________________________________
City__________________________________________State_____________Zip_____________
APPLICANT INFORMATION
DATE________________ Position applying for: Contractor Driver Contractor’s D river
NAME_________________________________________________________________________
PHONE ( )____________________ EMERGENCY PHONE ( )___________________
AGE_____________ DATE OF BIRTH_____________________SS#_____________________
(The Age Discrimination of Employment Act of 1967 prohibits discrimination on the basis of age with respect to individuals who are at least 40
but less than 70 years of age.)
PHYSICAL EXAM EXPIRATION DATE_____________________
CURRENT & PREVIOUS THREE YEARS ADDRE SSES :
___________________________________________________FROM________________TO____________________
___________________________________________________FROM________________TO____________________
___________________________________________________FROM________________TO____________________
HAVE YOU WORKED FOR THIS COMPANY BEFORE? _______Y es ________No
If yes, give dates: From_______________ To_________________
Reason for leaving? _______________________________________________________________________________
EDUCATION HISTORY:
Please circle the highest grade completed:
Grade school: 1 2 3 4 5 6 7 8 9 10 11 12
College: 1 2 3 4 Post Graduate: 1 2 3 4
EMPLOYMENT HISTORY:
Give a COMPLETE RECORD of all employment for the past three (3) years, including any unemployment or self
employment periods, and all commercial driving experience for the past ten (10) years.
Mo/Yr Mo/Yr Present or Last Employer
From____________To___________ Name_____________________________________________________________
Position Held_____________________Address_________________________________________________________
Reason for leaving___ _________________________________ _______Company phone ( )__________________
Were you subject to th e FMCSRs while employed here? ____________Y es _____________N o
Was your job designated as a safety-sensitive function in any DOT- regulated mode subject to the drug and alcohol
testing requirements of 49 CFR Part 40? _______________ Yes _______________No
Mo/Yr Mo/Yr Present or Last Employer
From____________To___________ Name_____________________________________________________________
Position Held_____________________Address_________________________________________________________
Reason for leaving___ _________________________________ _______Company phone ( )__________________
Were you subject to th e FMCSRs while employed here? ____________Y es _____________N o
Was your job designated as a safety-sensitive function in any DOT- regulated mode subject to the drug and alcohol
testing requirements of 49 CFR Part 40? _______________ Yes _______________No
2
Mo/Yr Mo/Yr Present or Last Employer
From____________To___________ Name_____________________________________________________________
Position Held_____________________Address_________________________________________________________
Reason for leaving___ _________________________________ _______Company phone ( )__________________
Were you subject to th e FMCSRs while employed here? ____________Y es _____________N o
Was your job designated as a safety-sensitive function in any DOT- regulated mode subject to the drug and alcohol
testing requirements of 49 CFR Part 40? _______________ Yes _______________No
Mo/Yr Mo/Yr Present or Last Employer
From____________To___________ Name_____________________________________________________________
Position Held_____________________Address_________________________________________________________
Reason for leaving___ _________________________________ _______Company phone ( )__________________
Were you subject to th e FMCSRs while employed here? ____________Y es _____________N o
Was your job designated as a safety-sensitive function in any DOT- regulated mode subject to the drug and alcohol
testing requirements of 49 CFR Part 40? _______________ Yes _______________No
Mo/Yr Mo/Yr Present or Last Employer
From____________To___________ Name_____________________________________________________________
Position Held_____________________Address_________________________________________________________
Reason for leaving___ _________________________________ _______Company phone ( )__________________
Were you subject to th e FMCSRs while employed here? ____________Y es _____________N o
Was your job designated as a safety-sensitive function in any DOT- regulated mode subject to the drug and alcohol
testing requirements of 49 CFR Part 40? _______________ Yes _______________No
Mo/Yr Mo/Yr Present or Last Employer
From____________To___________ Name_____________________________________________________________
Position Held_____________________Address_________________________________________________________
Reason for leaving___ _________________________________ _______Company phone ( )__________________
Were you subject to th e FMCSRs while employed here? ____________Y es _____________N o
Was your job designated as a safety-sensitive function in any DOT- regulated mode subject to the drug and alcohol
testing requirements of 49 CFR Part 40? _______________ Yes _______________No
Mo/Yr Mo/Yr Present or Last Employer
From____________To___________ Name_____________________________________________________________
Position Held_____________________Address_________________________________________________________
Reason for leaving___ _________________________________ _______Company phone ( )__________________
Were you subject to th e FMCSRs while employed here? ____________Y es _____________N o
Was your job designated as a safety-sensitive function in any DOT- regulated mode subject to the drug and alcohol
testing requirements of 49 CFR Part 40? _______________ Yes _______________No
(Attach additional sheets for 10-year history, if needed.)
3
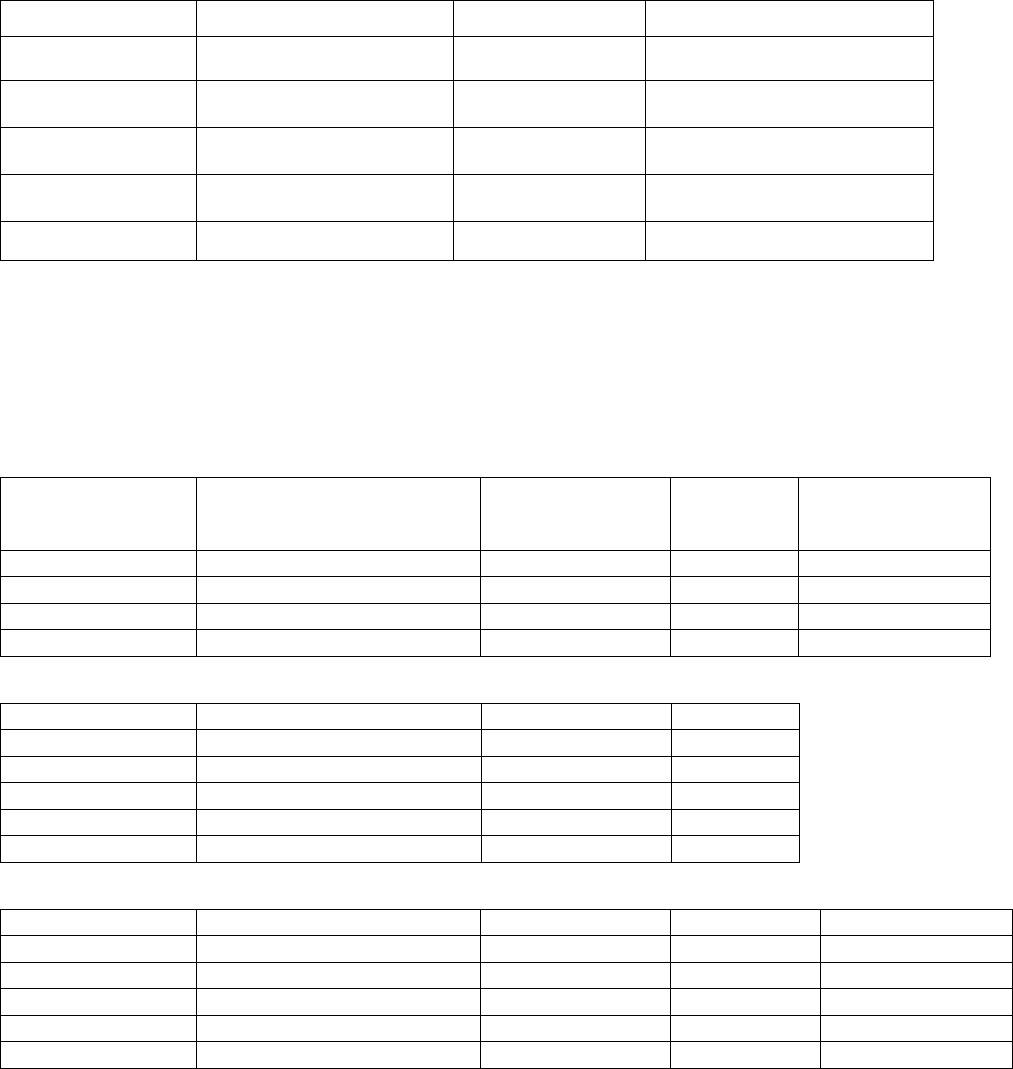
DRIVING EXPERIENCE
Class of Equipment
From
To
Approximate Number of Miles
Straight Truck
Tractor & Semi-
trailer
Tractor & two
trailers
Tractor & triple
trailers
Other
List states operated in, for the last five (5) years:_____________________________________ __________________
List special courses/training completed (PTD/DDC, HAZMAT, ETC)___ __________________ _________________
List any Safe Driving Awards you hold and from whom:_________________________________________________
Accident Record for past three (3) years: (attach sheet if more space is needed):
Date of Accident Nature of Accidents
Location of
Accident
# of
Fatalities # of People Injured
(Head on, rear end, etc)
Traffic Convictions and Forfeitures for the last three (3) years (other than parking violations):
Date Location Charge Penalty
Driver’s License (list each driver’s license held in the past three(3) years:
State License Type Endorsements Expiration Date
Have you ever been denied a license, permit or privilege to operate a motor veh icle? ________Yes ________No
Has any license, permit or privilege ever been suspended or revoked? ________Yes ________No
Is there any reason you might be unable to perform the functions of the job for which you have applied (as described in
the job description)? ________Yes _______No
Have you ever been convicted of a felony? ________Yes _______No
If the answer s to any questions listed above are “yes”, give details__________________________________________
4
Job References
List three (3) persons for references, ot her th an family members, who have knowled ge of y our safety habits.
Name________________________________Address_________________________________Phone_______________
Name________________________________Address_________________________________Phone_______________
Name________________________________Address_________________________________Phone_______________
To Be Read and Signed by Applicant:
It is agreed and understood that any mi srep resent at i o n gi ven on this appl i c at i on sh al l be considered an act of
dishonesty.
It is agreed and understood that the motor carrier or his agents may investigate the applicant’s background to obtain
any and all information of concern to applicant’s record, whether same is of record or not, and applicant releases
employers and person named herein from all liability for any damages on account of his furnishing such information.
It is also agreed and understood that under the Fair Credit Reporting Act, Public Law 91-508, I have been told that this
investigation may includ e an investigating Consumer Report, including information regarding my character, g en e ral
reputation, personal characteristics, and mode of living.
I agree to furnish such additional info rmation and complete such examinations as may be required to complete my
application file.
It is agreed and understood that this Application in no way obligates the motor carrier to employ or hire the applicant.
It is agreed and understood that if qualified and hired, I may be on a probationary period during which time I may be
disqualified without recourse.
This certifies that this applicatio n was completed by me, and that all entries on it and information in it are true and
complete to the best of my knowledge.
Applicant Signature_____________________________________________Date________________________
Remarks: (For office use only)
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________


