
Fillable Printable Blank Employment Verification Form
Fillable Printable Blank Employment Verification Form
Blank Employment Verification Form
DSHS 14-252(X) (REV. 05/2015)
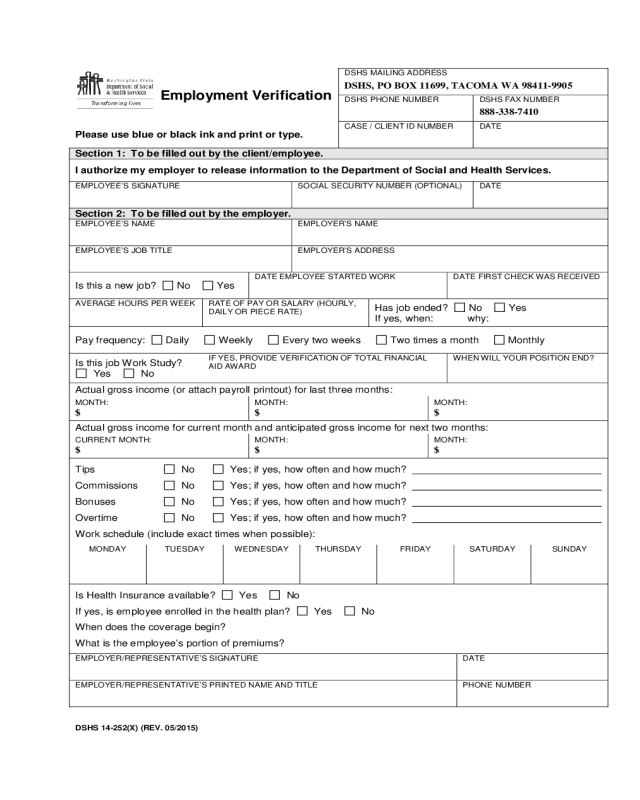
Employment Verification
DSHS MAILING ADDRESS
DSHS, PO BOX 11699, TACOMA WA 98411-9905
DSHS PHONE NUMBER
DSHS FAX NUMBER
888-338-7410
Please use blue or black ink and print or type.
CASE / CLIENT ID NUMBER
DATE
Section 1: To be filled out by the clie n t/emp loyee.
I authorize my employer to release information to the Department of Social and Health Services.
EMPLOYEE’S SIGNATURE
SOCIA L SE CURITY NUMBER (OPTIONAL)
DATE
Section 2: To be filled out by the employer.
EMPLOYEE’S NAME
EMPLOYER’S NAME
EMPLOYEE’S J O B TITLE
EMPLOYER’S ADDRESS
Is this a new job? No Yes
DATE EMPL O YEE STAR TED WOR K
DATE FIRST CHECK WAS RECEIVED
AVERA GE H O U R S PER WEEK
RATE OF PAY OR SALARY (HOURLY,
DAILY OR PIECE RATE)
Has job ended? No Yes
If yes, when: why:
Pay frequency: Daily Weekly Every two weeks Two times a month Monthly
Is this job Work Study?
Yes No
IF YES, PROVIDE VERIFICATION OF TOTAL FINANCIAL
AID A WARD
WHEN WILL YOUR POSITION END?
Actual gross income (or attach payroll printout) for last three months:
MONTH:
$
MONTH:
$
MONTH:
$
Actual gross income for current month and anticipated gross income for next two months:
CURRENT MONTH:
$
MONTH:
$
MONTH:
$
Tips No Ye s; i f yes, how often and how much?
Commissions No Yes; if yes, how often and how much?
Bonuses No Yes; if yes, how often and how much?
Overtime No Yes; if yes, how often and how much?
Work schedule (include exact times when possible):
MONDAY
TUESDAY
WEDNESDAY
THURSDAY
FRIDAY
SATURDAY
SUNDAY
Is Health Insurance available? Yes No
If yes, is emplo yee enro lle d in the health plan? Yes No
When does the coverage begin?
What is the employee’s portion of premiums?
EMPL O YER/RE PR ESENT ATIVE’S SIGN ATURE
DATE
EMPLOYER /R E PRESENTATIVE’S PR IN TED NAME AND TITLE
PHONE NUMBER


