
Fillable Printable Standard Employment Verification Form
Fillable Printable Standard Employment Verification Form
Standard Employment Verification Form

X
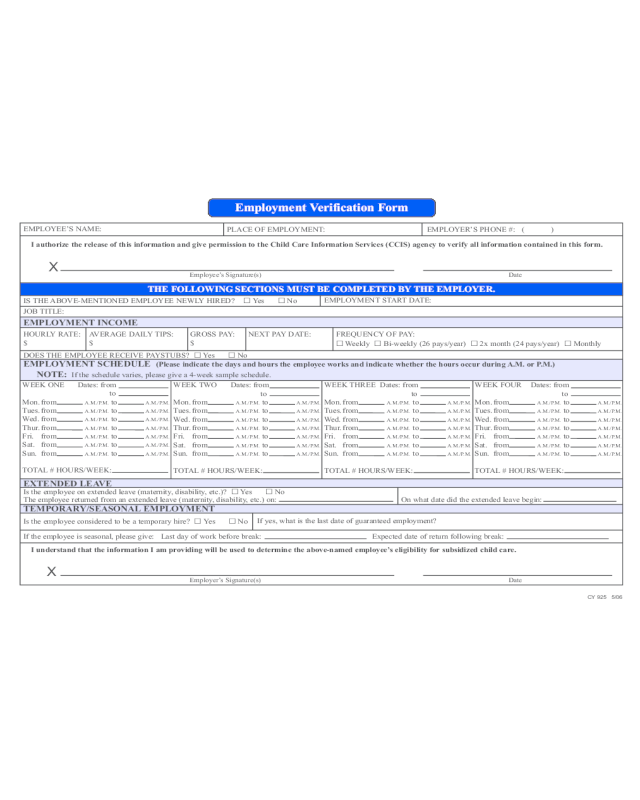
Employment Verification Form
EMPLOYEE’S NAME:
PLACE OF EMPLOYMENT:
EMPLOYER’S PHONE #:
I authorize the release of this information and give permission to the Child Care Information Services (CCIS) agency to verify all information contained in this form.
Employee’s Signature(s) Date
THE FOLLOWING SECTIONS MUST BE COMPLETED BY THE EMPLOYER.
IS THE ABOVE-MENTIONED EMPLOYEE NEWLY HIRED? �
Yes �
No
EMPLOYMENT START DATE:
JOB TITLE:
EMPLOYMENT INCOME
HOURLY RATE:
AVERAGE DAILY TIPS: GROSS PAY: NEXT PAY DATE:
�
� � �
( )
$
$ $
FREQUENCY OF PAY:
Weekly
Bi-weekly (26 pays/year)
2x month (24 pays/year)
Monthly
DOES THE EMPLOYEE RECEIVE PAYSTUBS? �
Yes �
No
EMPLOYMENT SCHEDULE
(Please indicate the days and hours the employee works and indicate whether the hours occur during A.M. or P.M.)
NOTE: If the schedule varies, please give a 4-week sample schedule.
WEEK ONE Dates: from
to
Mon. from
A.M./P.M. to A.M./P.M.
Tues. from A.M./P.M. to A.M./P.M.
Wed. from A.M./P.M. to A.M./P.M.
Thur. from A.M./P.M. to A.M./P.M.
Fri. from A.M./P.M. to A.M./P.M.
Sat. from A.M./P.M. to A.M./P.M.
Sun. from A.M./P.M. to A.M./P.M.
TOTAL # HOURS/WEEK:
WEEK TWO Dates: from
to
Mon. from
A.M./P.M. to A.M./P.M.
Tues. from
A.M./P.M. to A.M./P.M.
Wed. from A.M./P.M. to A.M./P.M.
Thur. from A.M./P.M. to A.M./P.M.
Fri. from A.M./P.M. to A.M./P.M.
Sat. from A.M./P.M. to A.M./P.M.
Sun. from A.M./P.M. to A.M./P.M.
TOTAL # HOURS/WEEK:
WEEK THREE Dates: from
to
Mon. from
A.M./P.M. to A.M./P.M.
Tues. from
A.M./P.M. to A.M./P.M.
Wed. from A.M./P.M. to A.M./P.M.
Thur. from A.M./P.M. to A.M./P.M.
Fri. from A.M./P.M. to A.M./P.M.
Sat. from A.M./P.M. to A.M./P.M.
Sun. from A.M./P.M. to A.M./P.M.
TOTAL # HOURS/WEEK:
WEEK FOUR Dates: from
to
Mon. from
A.M./P.M. to A.M./P.M.
Tues. from
A.M./P.M. to A.M./P.M.
Wed. from A.M./P.M. to A.M./P.M.
Thur. from A.M./P.M. to A.M./P.M.
Fri. from A.M./P.M. to A.M./P.M.
Sat. from A.M./P.M. to A.M./P.M.
Sun. from A.M./P.M. to A.M./P.M.
TOTAL # HOURS/WEEK:
EXTENDED LEAVE
Is the employee on extended leave (maternity, disability, etc.)? �
Yes �
No
The employee returned from an extended leave (maternity, disability, etc.) on: On what date did the extended leave begin:
TEMPORARY/SEASONAL EMPLOYMENT
Is the employee considered to be a temporary hire? �
Yes �
No
If yes, what is the last date of guaranteed employment?
If the employee is seasonal, please give: Last day of work before break: Expected date of return following break:
I understand that the information I am providing will be used to determine the above-named employee’s eligibility for subsidized child care.
Employer’s Signature(s) Date
X
CY 925 5/06
Employment Verification Form
Dear Employer:
One of your employees has requested assistance paying his/her child care costs. We must verify his/her employment with you. This information will
help us determine if this employee is eligible for the subsidized child care program. The form can be returned to the employee or mailed directly to the
Child Care Information Services (CCIS) agency.
An authorized COMPANY REPRESENTATIVE (not the employee) must complete this form.
We must have an accurate record of your employee’s work schedule. Please complete the information on the back of this page. It is very important that
the hours shown are specific and defined as either A.M. or P.M. (For example, 7:30 a.m. - 3:30 p.m.). If the employee’s schedule varies, please give a
4-week sample schedule. You do not need to give a 4-week sample schedule unless the employee’s schedule varies from week to week.
Thank you for your time and assistance. If you have any questions about how to complete this form, please contact the CCIS listed below.
CCIS:
CY 868 5/06
CY 925 4/06


