
Fillable Printable Cdl Diabetes Waiver Interim Assessment Form
Fillable Printable Cdl Diabetes Waiver Interim Assessment Form
Cdl Diabetes Waiver Interim Assessment Form
Name:
NCDL#
Date:
Page 1 of 1
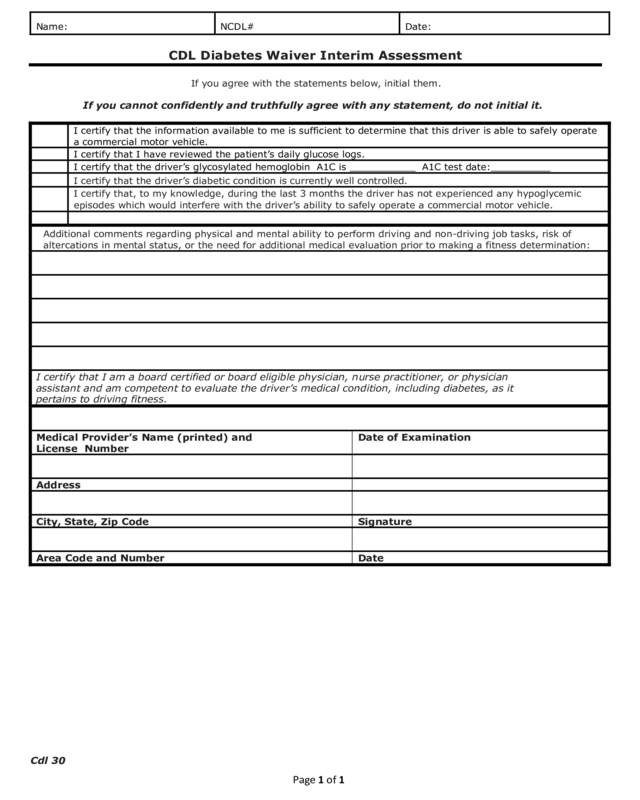
CDL Diabetes Waiver Interim Assessment
If you agree with the statements below, initial them.
If you cannot confidently and truthfully agree with any statement, do not initial it.
I certify that the information available to me is sufficient to determine that this driver is able to safely operate
a commercial motor vehicle.
I certify that I have reviewed the patient’s daily glucose logs.
I certify that the driver’s glycosylated hemoglobin A1C is ___________ A1C test date:__________
I certify that the driver’s diabetic condition is currently well controlled.
I certify that, to my knowledge, during the last 3 months the driver has not experienced any hypoglycemic
episodes which would interfere with the driver’s ability to safely operate a commercial motor vehicle.
Additional comments regarding physical and mental ability to perform driving and non-driving job tasks, risk of
altercations in mental status, or the need for additional medical evaluation prior to making a fitness determination:
I certify that I am a board certified or board eligible physician, nurse practitioner, or physician
assistant and am competent to evaluate the driver’s medical condition, including diabetes, as it
pertains to driving fitness.
Medical Provider’s Name (printed) and
License Number
Date of Examination
Address
City, State, Zip Code
Signature
Area Code and Number
Date
Cdl 30


