
Fillable Printable Certificate Of Clinical Training - Form L5
Fillable Printable Certificate Of Clinical Training - Form L5
Certificate Of Clinical Training - Form L5
BUSINESS , CONSUMER SERVICES, AND H O US I NG AGENCY - De p ar tment of Consumer Affair s EDMUND G. BROWN JR., Governor
MEDICAL BOARD OF CALIFORNIA
Licensing Program
07A-100 (Revised 7/2016)
2005 Evergreen Street, Suite 1200, Sacramento, CA 95815-3831 (916) 263-2382 (800) 63 3-2322 FAX: (916) 263-2487 www.mbc.ca.gov
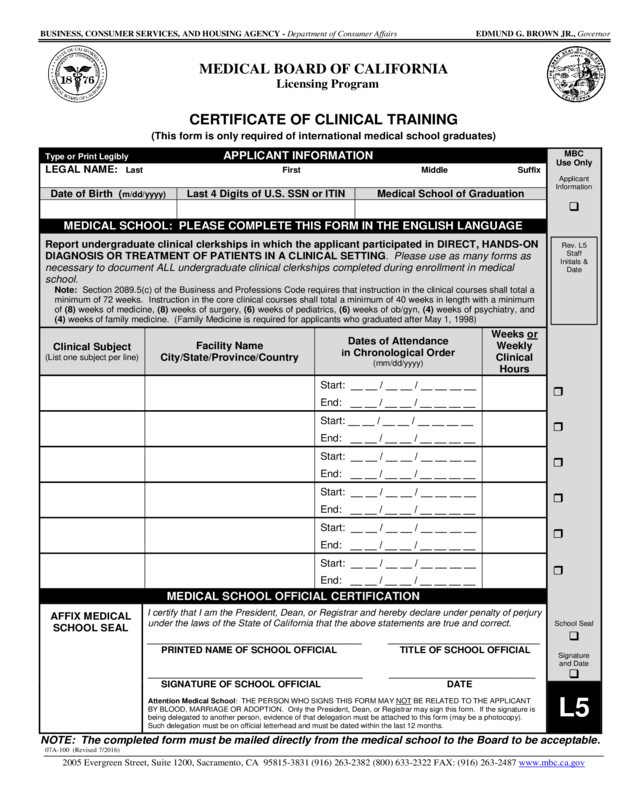
CERTIFI CATE OF CLINICAL TRAINING
(This form is only required of interna tional medical school graduates)
Type or Print Legibly APPLICANT INFORMATION
MBC
Use Only
Applicant
Information
School Seal
Signature
and Date
LEGAL NAME: Last First Middle Suffix
Date of Birth (m/dd/yyyy)
Last 4 Digits of U.S. SSN or ITIN
Medical Sch o o l of Graduation
MEDICAL SCHOOL: PLEASE COMPLETE THIS FO RM IN THE ENGLISH LANGUAGE
Report undergraduate clinical clerkships in which the applicant participated in DIRECT, HANDS-ON
DIAGNOSIS OR TREATMENT OF PATIENTS IN A CLINICAL SETTING. Please use as many forms as
necessary to document ALL undergraduate clinical clerkships completed during enrollment in medical
school.
Note: S ection 2089.5(c) of the B usiness and Prof essions Code requires t hat instr uction in the clinical courses shall total a
minim um of 72 w eeks . Inst r uction i n the c or e cl i nical cours es shall t otal a mi nim um of 40 weeks i n lengt h wi th a m ini mum
of (8) week s of medic ine, (8) weeks of sur gery, (6) weeks of pedi atri cs, (6) weeks of ob/gyn, (4) weeks of ps ychiat ry, and
(4) w eeks of fam ily medicine. (Family Medicine is r equired for applicants who graduated after M ay 1, 1998)
Clinical Subject
(List one subject per li ne)
Facility Name
City/State/Province/Country
Dates of Attendance
in Chronologi cal Order
(mm/dd/yyyy)
Weeks or
Weekly
Clinical
Hours
Start: __ __ / __ __ / __ __ __ __
End: __ __ / __ __ / __ __ __ __
Start: __ __ / __ __ / __ __ __ __
End: __ __ / __ __ / __ __ __ __
Start: __ __ / __ __ / __ __ __ __
End: __ __ / __ __ / __ __ __ __
Start: __ __ / __ __ / __ __ __ __
End:
__ __ / __ __ / __ __ __ __
Start: __ __ / __ __ / __ __ __ __
End: __ __ / __ __ / __ __ __ __
Start: __ __ / __ __ / __ __ __ __
End: __ __ / __ __ / __ __ __ __
MEDICAL SCHOOL OFFICIAL CERT IFICATION
AFFIX MEDICAL
SCHOOL SEAL
I certify that I am the President, Dean, or Registrar and hereby declare under penalty of perjury
under the laws of the State of California that the above statements are true and correct.
_________________________________________ _____________________________
PRINTED NAME OF SCHOOL OFFICIAL TITLE OF SCHOOL OFFICIAL
_________________________________________ ____________________________
SIGNATURE OF SCHOOL OFFICIAL DATE
Attention Medical School: THE PERSON WHO SIGNS THIS FORM MAY NOT BE RELATED TO THE APPLICANT
BY BLOOD, MARRIAGE OR ADOPTION. Only the President, Dean, or Registrar may sign this form. If the signature is
being delegated to another person, evidence of that delegation must be attached to this form (may be a photocopy).
Such delegation must be on official letterhead and must be dated within the last 12 months.
L5
NOTE: The complet ed form must be mailed directly from the medical school to the Board to be ac ceptable.
Rev. L5
Staff
Initials &
Date


