
Fillable Printable Claim For Refund Of Excess Ca Sdi Insurance Deductions (De 1964)
Fillable Printable Claim For Refund Of Excess Ca Sdi Insurance Deductions (De 1964)
Claim For Refund Of Excess Ca Sdi Insurance Deductions (De 1964)
DE 1964 Rev. 32 (12-16) (INTERNET) Page 1 of 2 CU
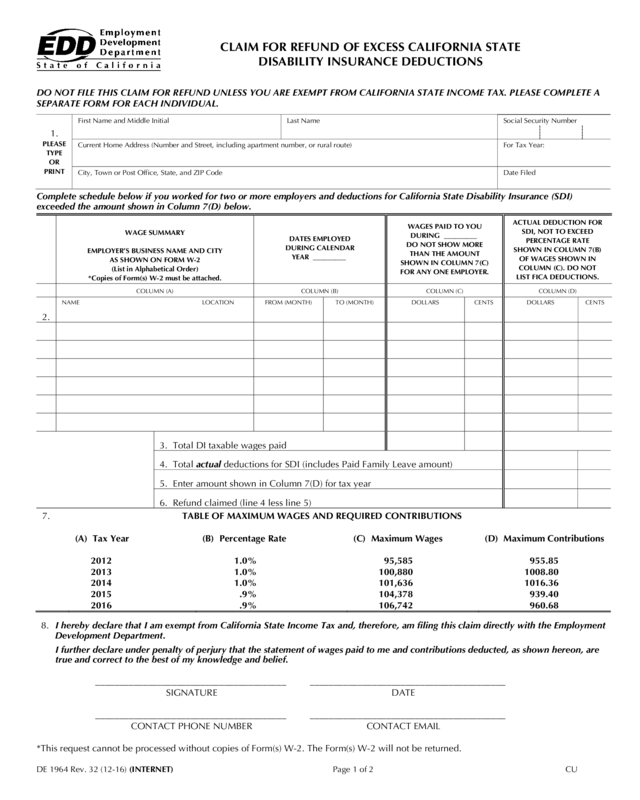
CLAIM FOR REFUND OF EXCESS CALIFORNIA STATE
DISABILITY INSURANCE DEDUCTIONS
DO NOT FILE THIS CLAIM FOR REFUND UNLESS YOU ARE EXEMPT FROM CALIFORNIA STATE INCOME TAX. PLEASE COMPLETE A
SEPARATE FORM FOR EACH INDIVIDUAL.
First Name and Middle Initial Last Name Social Security Number
1.
PLEASE
TYPE
OR
Current Home Address (Number and Street, including apartment number, or rural route) For Tax Year:
PRINT
City, Town or Post Office, State, and ZIP Code Date Filed
Complete schedule below if you worked for two or more employers and deductions for California State Disability Insurance (SDI)
exceeded the amount shown in Column 7(D) below.
WAGE SUMMARY
EMPLOYER’S BUSINESS NAME AND CITY
AS SHOWN ON FORM W-2
(List in Alphabetical Order)
*Copies of Form(s) W-2 must be attached.
DATES EMPLOYED
DURING CALENDAR
YEAR _________
WAGES PAID TO YOU
DURING _________
DO NOT SHOW MORE
THAN THE AMOUNT
SHOWN IN COLUMN 7(C)
FOR ANY ONE EMPLOYER.
ACTUAL DEDUCTION FOR
SDI, NOT TO EXCEED
PERCENTAGE RATE
SHOWN IN COLUMN 7(B)
OF WAGES SHOWN IN
COLUMN (C). DO NOT
LIST FICA DEDUCTIONS.
COLUMN (A) COLUMN (B) COLUMN (C) COLUMN (D)
2.
NAME LOCATION FROM (MONTH) TO (MONTH) DOLLARS CENTS DOLLARS CENTS
3. Total DI taxable wages paid
4. Total actual deductions for SDI (includes Paid Family Leave amount)
5. Enter amount shown in Column 7(D) for tax year
6. Refund claimed (line 4 less line 5)
7.
TABLE OF MAXIMUM WAGES AND REQUIRED CONTRIBUTIONS
(A) Tax Year
(B) Percentage Rate
(C) Maximum Wages
(D) Maximum Contributions
2012
1.0%
95,585
955.85
2013
1.0%
100,880
1008.80
2014
1.0%
101,636
1016.36
2015
.9%
104,378
939.40
2016
.9%
106,742
960.68
8. I hereby declare that I am exempt from California State Income Tax and, therefore, am filing this claim directly with the Employment
Development Department.
I further declare under penalty of perjury that the statement of wages paid to me and contributions deducted, as shown hereon, are
true and correct to the best of my knowledge and belief.
________________________________________ _________________________________________
SIGNATURE DATE
________________________________________ _________________________________________
CONTACT PHONE NUMBER CONTACT EMAIL
*This request cannot be processed without copies of Form(s) W-2. The Form(s) W-2 will not be returned.
DE 1964 Rev. 32 (12-16) (INTERNET) Page 2 of 2
INSTRUCTIONS
CLAIM FOR REFUND OF EXCESS CALIFORNIA STATE
DISABILITY INSURANCE DEDUCTIONS
CLAIM MUST BE BASED ON CALENDAR YEAR WAGES
A valid State Disability Insurance (SDI) refund claim filed directly with the Employment Development Department on this form must meet ALL
of the following conditions:
1. Claimant worked for two or more employers subject to withholding California SDI.
2. Deductions for California SDI were made from calendar year wages.
3. Such deductions exceed the statutory limits.
4. Claimant declares by signature to exemption from California State Income Tax.
WHERE TO FILE CLAIM
Employment Development Department, PO Box 826880, Special Processes Group MIC 13, Sacramento, CA 94280-0001.
WHEN TO FILE CLAIM
Claims for credit or refund of California SDI overpayment must be filed within three years after the end of the calendar year in which the
excess deductions were made. The claim must be based on the calendar year in which the wages were received.
AMENDED CLAIMS
Amended claims must be marked as “Amended” (if not, they will be returned to claimant) and forwarded to the Employment Development
Department, PO Box 826880, Special Processes Group MIC 13, Sacramento, CA 94280-0001.
INFORMATION FOR COMPLETING WAGE SUMMARY SCHEDULE
1. The SDI deductions are shown on Form(s) W-2, employer statements, and check stubs.
2. Most federal, state, and local government agencies are not required to deduct California SDI. Do not include these wages in your claim
unless Disability Insurance deductions were actually made.
3. Do not include in your claim:
a. Deductions made from your wages for Social Security and Medicare (FICA), or federal and state income tax withheld from your wages.
b. Deductions made from wages earned in states other than California, unless such wages were reported to the State of California.
c. Seaman's wages that come under the jurisdiction of states other than California.
4. Self-employed persons – Enter in Column (A) "Covered under California Unemployment Insurance Code Section 708 or 708.5" and
complete Column (B). Failure to enter this information will result in rejection of your claim on initial review.
INSTRUCTIONS FOR COMPLETING DE 1964
1. Enter all information requested in section 1.
2. Enter employer information:
Column (A) – All employers and location of job sites, attach Form(s) W-2.
Column (B) – The calendar year dates employed by employer in Column (A).
Column (C) – Wages up to annual maximum shown in Section 7(C) paid to you by individual Column (A) employers.
Column (D) – Enter actual amount of SDI withheld. Do not exceed the percentage rate shown in Section 7(B) of wages in
Column (C).
3. Enter total SDI taxable wages paid.
4. Enter total of all SDI deductions withheld by each employer in Column (D). This amount must be verified by attached Form W-2 copies
showing SDI amounts withheld or a statement from the employer indicating the amount of SDI withheld.
5. Enter maximum contribution for tax year (see Column 7D).
6. Enter amount of refund claimed (line 4 less line 5).
7. Table of Maximum Wages and Required Contributions (reference table only).
8. Read and sign this declaration, which states you are exempt from California State Income Tax. Without your signature, your claim will be
rejected.
9. Enter your phone number and date.
ASSISTANCE
If you need assistance in completing this claim, contact the Excess State Disability Insurance Unit of the Employment Development
Department, PO Box 826880, Special Processes Group MIC 13, Sacramento, CA 94280-0001, 916-654-8333.


