
Fillable Printable Credit Authorization to Indiana University for Direct Bank Deposit Service - Indiana University
Fillable Printable Credit Authorization to Indiana University for Direct Bank Deposit Service - Indiana University
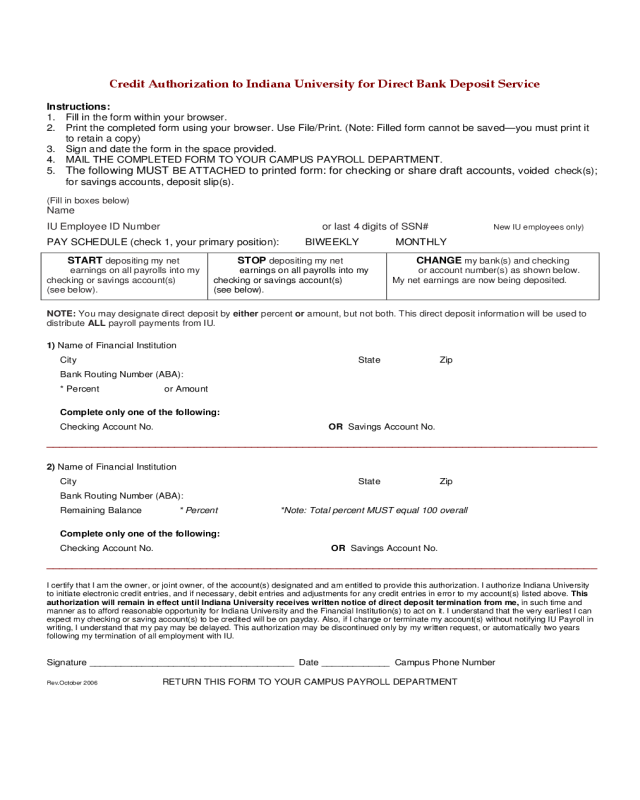
Credit Authorization to Indiana University for Direct Bank Deposit Service - Indiana University

CreditAuthorizationtoIndianaUniversityforDirectBankDepositService
Instructions:
1. Fill in the form within your browser.
2. Print the completed form using your bro wser. Use Fil e/Print. (Note : Filled form cannot be saved—you mu st print it
to retain a copy)
3. Sign and date the form in the sp ace provided.
4. MAIL THE COMPLETED FORM TO YOUR CAMPUS PAYROLL DEPARTME NT.
5.
The following MUST BE ATTACHED to printed form: for checking or share draft accounts, voided check(s);
for savings accounts, deposit slip (s).
(Fill in boxes below)
Name
IU Employee ID Number or last 4 digits of SSN# New IU employees only)
PAY SCHEDULE (check 1, your primary position): BIWEEKLY MONTHLY
START depositing m y net
earnings on all payrolls i nto my
checking or savings account(s)
(see below).
STOP depositing my net
earnings on all payrolls into my
checking or savings account(s)
(see below).
CHANGE my bank(s) and checking
or account number(s) as shown below.
My net earnings are now being deposited.
NOTE: You may designate direct deposit by either percent or amount, but not both. This direct deposit information will be used to
distribute ALL payroll pa yments from IU.
1) Name of Financi al Institutio n
City State Zip
Bank Routing Number (ABA):
* Percent or Amount
Complete only one of the following:
Checking Account No. OR Savings Account No.
______________________________________________________________________________________
2) Name of Financi al Institutio n
City State Zip
Bank Routing Number (ABA):
Remaining Balance * Percent *Note: Total percent MUST equal 100 overall
Complete only one of the following:
Checking Account No. OR Savings Account No.
______________________________________________________________________________________
I certify that I am the owner, or joint owner, of the account(s) designated and am entitled to provide this authorization. I authorize Indiana University
to initiate electronic credit entries, and if necessary, debit entries and adjustments for any credit entries in error to my account(s) listed above. This
authorization will remain in effect until Indiana University receives written notice of direct deposit termination from me, in such time and
manner as to afford reasonable opportunity for Indiana University and the Financial Institution(s) to act on it. I understa nd that the very earliest I can
expect my checking or saving account(s) to be credited will be on payday. Also, if I change or terminate my account(s) without notifying IU Payroll in
writing, I understand that my pay may be delayed. This authorization ma y be discontinued only by my written request, or automatically two years
following my termination of all employment with IU.
Signature ____________ ________________ ___________ Date _______ ______ Campus Phone Number
Rev.October 2006 RETURN THIS FORM TO YOUR CAMPUS PAYROLL DE PARTMENT


