
Fillable Printable De2063F
Fillable Printable De2063F
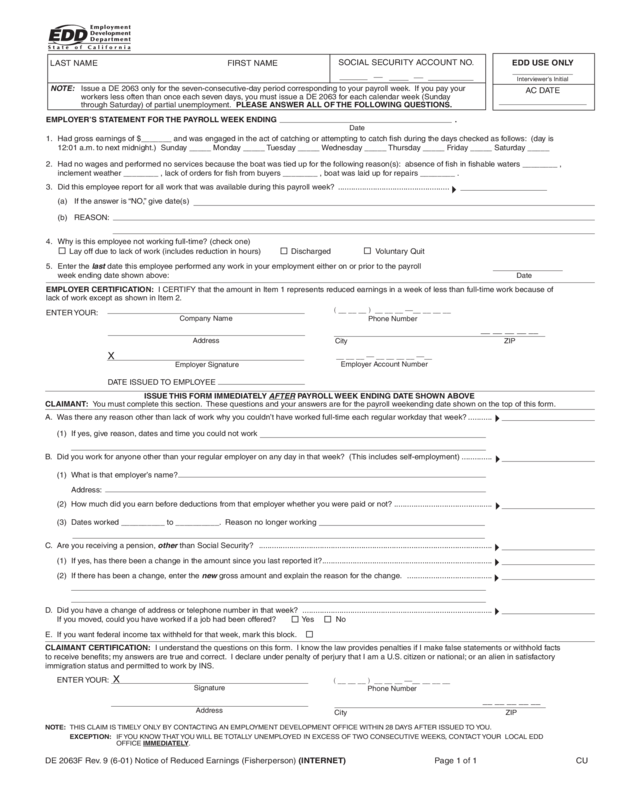
De2063F
LAST NAME
NOTE: Issue a DE 2063 only for the seven-consecutive-day period corresponding to your payroll week. If you pay your
workers less often than once each seven days, you must issue a DE 2063 for each calendar week (Sunday
through Saturday) of partial unemployment. PLEASE ANSWER ALL OF THE FOLLOWING QUESTIONS.
SOCIAL SECURITY ACCOUNT NO.
EDD USE ONLY
Interviewer’s Initial
AC DATE
EMPLOYER’S STATEMENT FOR THE PAYROLL WEEK ENDING .
Date
1. Had gross earnings of $_______ and was engaged in the act of catching or attempting to catch fi sh during the days checked as follows: (day is
12:01 a.m. to next midnight.) Sunday _____ Monday _____ Tuesday _____ Wednesday _____ Thursday _____ Friday _____ Saturday _____
2. Had no wages and performed no services because the boat was tied up for the following reason(s): absence of fi sh in fi shable waters ________ ,
inclement weather ________ , lack of orders for fi sh from buyers ________ , boat was laid up for repairs ________ .
3. Did this employee report for all work that was available during this payroll week? ...................................................
(a) If the answer is “NO,” give date(s)
(b) REASON:
4. Why is this employee not working full-time? (check one)
Lay off due to lack of work (includes reduction in hours) Discharged Voluntary Quit
5. Enter the last date this employee performed any work in your employment either on or prior to the payroll
week ending date shown above:
Date
EMPLOYER CERTIFICATION: I CERTIFY that the amount in Item 1 represents reduced earnings in a week of less than full-time work because of
lack of work except as shown in Item 2.
ENTER YOUR:
Company Name
Address
City ZIP
( __ __ __ ) __ __ __ —__ __ __ __
Phone Number
__ __ __ __ __
__ __ __ — __ __ __ __ —__
Employer Account Number
Employer Signature
X
DATE ISSUED TO EMPLOYEE
ISSUE THIS FORM IMMEDIATELY AFTER PAYROLL WEEK ENDING DATE SHOWN ABOVE
CLAIMANT: You must complete this section. These questions and your answers are for the payroll weekending date shown on the top of this form.
A. Was there any reason other than lack of work why you couldn’t have worked full-time each regular workday that week? ...........
(1) If yes, give reason, dates and time you could not work
B. Did you work for anyone other than your regular employer on any day in that week? (This includes self-employment) ..............
(1) What is that employer’s name?
Address:
(2) How much did you earn before deductions from that employer whether you were paid or not? .............................................
(3) Dates worked __________ to __________. Reason no longer working
C. Are you receiving a pension, other than Social Security? ...........................................................................................................
(1) If yes, has there been a change in the amount since you last reported it? ..............................................................................
(2) If there has been a change, enter the new gross amount and explain the reason for the change. .......................................
D. Did you have a change of address or telephone number in that week? .......................................................................................
If you moved, could you have worked if a job had been offered? Yes No
E. If you want federal income tax withheld for that week, mark this block.
CLAIMANT CERTIFICATION: I understand the questions on this form. I know the law provides penalties if I make false statements or withhold facts
to receive benefi ts; my answers are true and correct. I declare under penalty of perjury that I am a U.S. citizen or national; or an alien in satisfactory
immigration status and permitted to work by INS.
ENTER YOUR:
4
NOTE: THIS CLAIM IS TIMELY ONLY BY CONTACTING AN EMPLOYMENT DEVELOPMENT OFFICE WITHIN 28 DAYS AFTER ISSUED TO YOU.
EXCEPTION: IF YOU KNOW THAT YOU WILL BE TOTALLY UNEMPLOYED IN EXCESS OF TWO CONSECUTIVE WEEKS, CONTACT YOUR LOCAL EDD
OFFICE IMMEDIATELY.
__ __ __ __ __
X
( __ __ __ ) __ __ __ —__ __ __ __
Phone Number
Signature
Address
City ZIP
4
4
4
4
4
4
4
FIRST NAME
DE 2063F Rev. 9 (6-01) Notice of Reduced Earnings (Fisherperson) (INTERNET) Page 1 of 1 CU


