
Fillable Printable Death Report Form - California
Fillable Printable Death Report Form - California
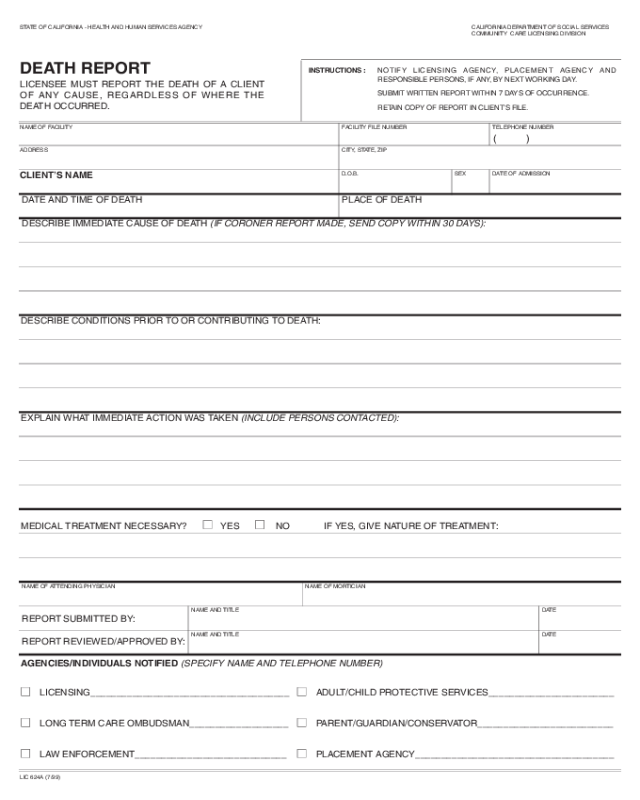
Death Report Form - California
STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AGENCY CALIFORNIA DEPARTMENT OF SOCIAL SERVICES
COMMUNITY CARE LICENSING DIVISION
DEATH REPORT
LICENSEE MUST REPORT THE DEATH OF A CLIENT
OF ANY CAUSE, REGARDLESS OF WHERE THE
DEATH OCCURRED.
INSTRUCTIONS : NOTIFY LICENSING AGENCY, PLACEMENT AGENCY AND
RESPONSIBLE PERSONS, IF ANY, BY NEXT WORKING DAY.
SUBMIT WRITTEN REPORT WITHIN 7 DAYS OF OCCURRENCE.
RETAIN COPY OF REPORT IN CLIENT’S FILE.
NAME OF FACILITY FACILITY FILE NUMBER
CITY, STATE, ZIP
D.O.B.
DATE AND TIME OF DEATH
DESCRIBE IMMEDIATE CAUSE OF DEATH (IF CORONER REPORT MADE, SEND COPY WITHIN 30 DAYS):
DESCRIBE CONDITIONS PRIOR TO OR CONTRIBUTING TO DEATH:
EXPLAIN WHAT IMMEDIATE ACTION WAS TAKEN (INCLUDE PERSONS CONTACTED):
MEDICAL TREATMENT NECESSARY?
■■ YES ■■ NO IF YES, GIVE NATURE OF TREATMENT:
PLACE OF DEATH
SEX DATE OF ADMISSION
TELEPHONE NUMBER
( )
ADDRESS
CLIENT’S NAME
LIC 624A (7/99)
NAME OF ATTENDING PHYSICIAN
REPORT SUBMITTED BY:
REPORT REVIEWED/APPROVED BY:
NAME OF MORTICIAN
NAME AND TITLE
NAME AND TITLE
DATE
DATE
AGENCIES/INDIVIDUALS NOTIFIED (SPECIFY NAME AND TELEPHONE NUMBER)
■■ LICENSING______________________________________ ■■ ADULT/CHILD PROTECTIVE SERVICES________________________
■■ LONG TERM CARE OMBUDSMAN___________________ ■■ PARENT/GUARDIAN/CONSERVATOR__________________________
■■ LAW ENFORCEMENT_____________________________ ■■ PLACEMENT AGENCY______________________________________


