
Fillable Printable Direct Deposit Authorization Form - Colorado
Fillable Printable Direct Deposit Authorization Form - Colorado
Direct Deposit Authorization Form - Colorado
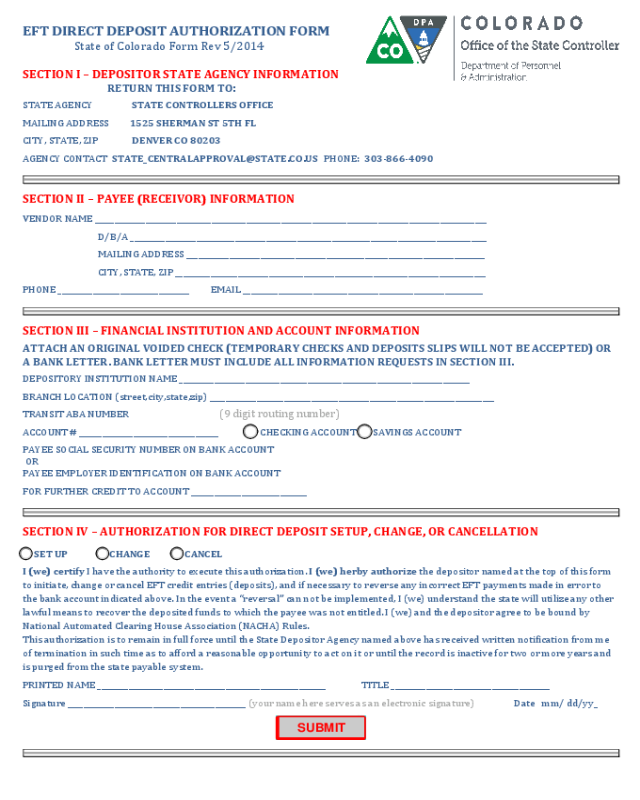
EFT DIRECT DEPOSIT AUTHORIZATION FORM
State of Colorado Form Rev 5/2014
SECTION I – DEPOSITOR STATE AGENCY INFORMATION
RETURN THIS FORM TO:
STATE AGENCY STATE CONTROLLERS OFFICE
MAILING ADDRESS 1525 SHERMAN ST 5TH FL
CITY, STATE, ZIP DENVER CO 80203
SECTION II – PAYEE (RECEIVOR) INFORMATION
VENDOR NAME _____________________________________________________________________________________________________
D/B/A ____________________________________________________________________________________________
MAILING ADDRESS _____________________________________________________________________________
CITY, STATE, ZIP ________________________________________________________________________________
PHONE __________________________________ EMAIL ______________________________________________________________
SECTION III – FINANCIAL INSTITUTION AND ACCOUNT INFORMATION
ATTACH AN ORIGINAL VOIDED CHECK (TEMPORARY CHECKS AND DEPOSITS SLIPS WILL NOT BE ACCEPTED) OR
A BANK LETTER. BANK LETTER MUST INCLUDE ALL INFORMATION REQUESTS IN SECTION III.
DEPOSITORY INSTITUTION NAME ___________________________________________________________________________
BRANCH LOCATION (street,city,state,zip) _________________________________________________________________________
TRANSIT ABA NUMBER
ACCOUNT # _
___________________________________ CHECKING ACCOUNT SAVINGS ACCOUNT
PAYEE SOCIAL SECURITY NUMBER ON BANK ACCOUNT
OR
PAYEE EMPLOYER IDENTIFICATION ON BANK ACCOUNT
FOR FURTHER CRED
IT TO ACCOUNT ______________________________
SECTION IV – AUTHORIZATION FOR DIRECT DEPOSIT SETUP, CHANGE, OR CANCELLATION
SET UP CHANGE CANCEL
I (we) certify I have the authority to execute this authorization. I (we) herby authorize the depositor named at the top of this form
to initiate, change or cancel EFT credit entries (deposits), and if necessary to reverse any incorrect EFT payments made in error to
the bank account indicated above. In the event a “reversal” can not be implemented, I (we) understand the state will utilize any other
lawful means to recover the deposited funds to which the payee was not entitled. I (we) and the depositor agree to be bound by
National Automated Clearing House Association (NACHA) Rules.
This authorization is to remain in full force until the State Depositor Agency named above has received written notification from me
of termination in such time as to afford a reasonable opportunity to act on it or until the record is inactive for two or more years and
is purged from the state payable system.
PRINTED NAME ___________________________________________________________ TITLE _________________________________________
Signature
______________________________________________ (your name here serves as an electronic signature)
Date mm/ dd/yy_
(9 digit routing number)


