
- Direct Deposit Authorization Agreement - Alabama
- Direct Deposit of Annuity Payments - Pennsylvania
- Direct Deposit Authorization - Florida State University
- Direct Deposit Authorization Sample Form - Indiana
- Direct Deposit Authorization - Arizona
- In-home Supportive Services Provider Direct Deposit Enrollment/Change/Cancellation Form - California
Fillable Printable Direct Deposit Authorization Form - Indiana University Health
Fillable Printable Direct Deposit Authorization Form - Indiana University Health
Direct Deposit Authorization Form - Indiana University Health

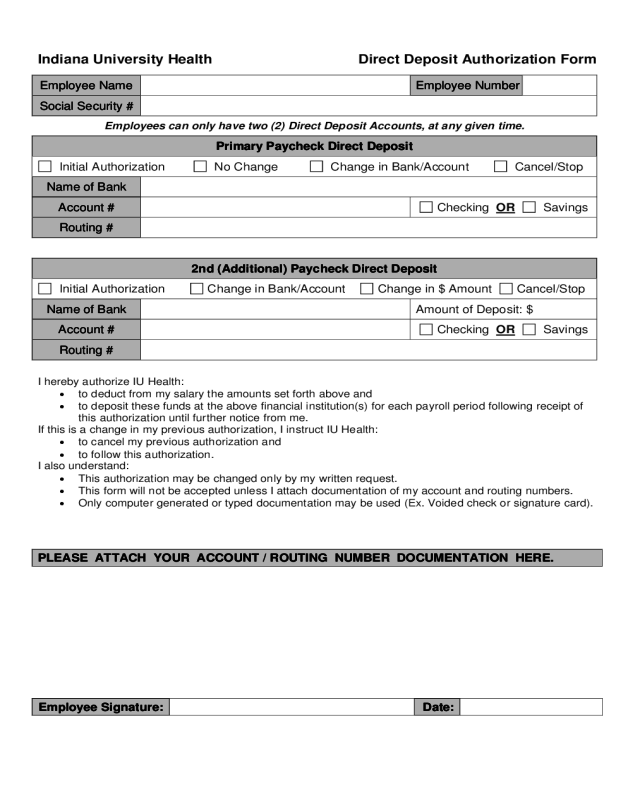
Indiana University Health Direct Deposit Authorization Form
Employee Name Employee Number
Social Security #
Employees can only have two (2) Direct Deposit Accounts, at any given time.
Primary Paycheck Direct Deposit
Initial Authorization No Change Change in Bank/Account Cancel/Stop
Name of Bank
Account # Checking OR Savings
Routing #
2nd (Additional) Paycheck Direct Deposit
Initial Authorization Change in Bank/Account Change in $ Amount Cancel/Stop
Name of Bank Amount of Deposit: $
Account # Checking OR Savings
Routing #
I hereby authorize IU Health:
• to deduct from my salary the amounts set forth above and
• to deposit these funds at the above financial institution(s) for each payroll period following receipt of
this authorization until further notice from me.
If this is a change in my previous authorization, I instruct IU Health:
• to cancel my previous authorization and
• to follow this authorization.
I also understand:
• This authorization may be changed only by my written request.
• This form will not be accepted unless I attach documentation of my account and routing numbers.
• Only computer generated or typed documentation may be used (Ex. Voided check or signature card).
PLEASE ATTACH YOUR ACCOUNT / ROUTING NUMBER DOCUMENTATION HERE.
Employee Signature: Date:


