
Fillable Printable Doh-4453 Duplicate Card Form
Fillable Printable Doh-4453 Duplicate Card Form
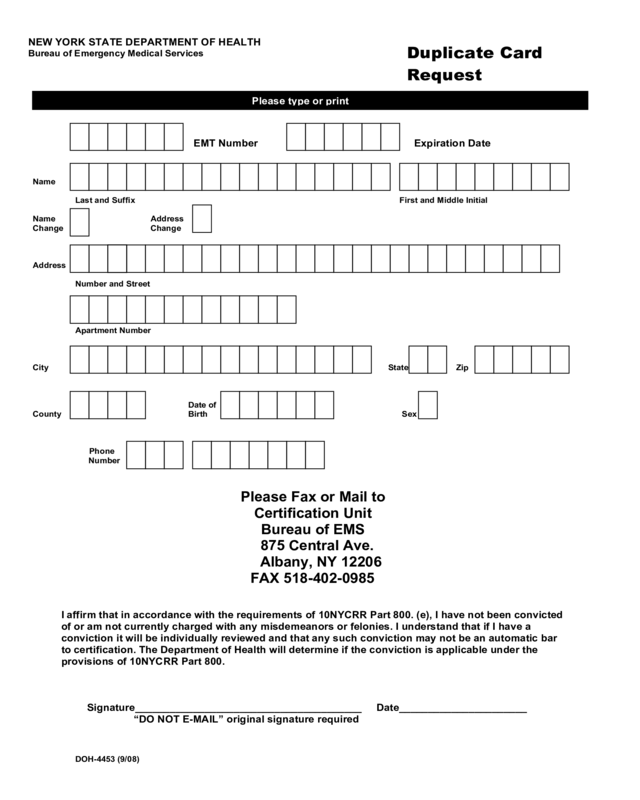
Doh-4453 Duplicate Card Form
NEW YORK STATE DEPARTMENT OF HEALTH
Bureau of Emergency Medical Services
DOH-4453 (9/08)
EMT Number Expiration Date
Name
Last and Suffix First and Middle Initial
Name Address
Change Change
Address
Number and Street
Apartment Number
City State Zip
Date of
County Birth Sex
Phone
Number
Please Fax or Mail to
Certification Unit
Bureau of EMS
875 Central Ave.
Albany, NY 12206
F
AX 518-402-0985
I affirm that in accordance with the requirements of 10NYCRR Part 800. (e), I have not been convicted
of or am not currently charged with any misdemeanors or felonies. I understand that if I have a
conviction it will be individually reviewed and that any such conviction may not be an automatic bar
to certification. The Department of Health will determine if the conviction is applicable under the
provisions of 10NYCRR Part 800.
Signature_______________________________________ Date______________________
“DO NOT E-MAIL” original signature required
Duplicate Card
Request
Please type or print


