
- Contractor's Certificate of Workers' Compensation Insurance - Virginia
- S.C. Workers' Compensation Commission First Report of Injury or Illness - Washington
- Application for Ohio Workers' Compensation Coverage
- Workers' Injury Reports Form - Maryland
- N.C. Workers' Compensation Notice to Injured Workers and Employees - North Carolina
- Worker's Compensation Information - Colorado
Fillable Printable Employee's Notice of Claim and/or Request for Hearing - South Carolina
Fillable Printable Employee's Notice of Claim and/or Request for Hearing - South Carolina
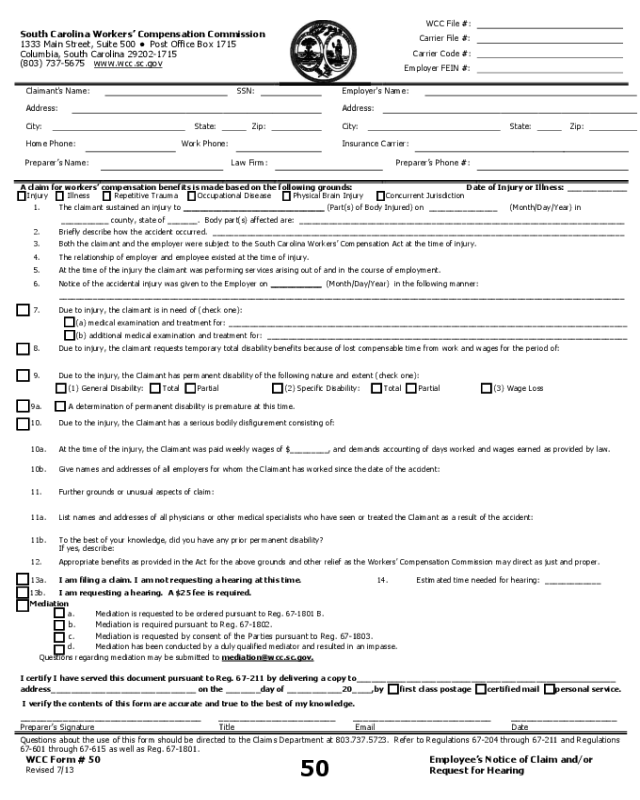
Employee's Notice of Claim and/or Request for Hearing - South Carolina
South Carolina Workers’ Compensation Commission
1333 Main Street, Suite 500 ● Post Office Box 1715
Columbia, South Carolina 29202-1715
(803) 737-5675 www.wcc.sc.gov
WCC File #:
Carrier File #:
Carrier Code #:
Employer FEIN #:
Claimant's Name:
SSN:
Address:
City:
State:
Zip:
Home Phone:
Work Phone:
Employer's Name:
Address:
City:
State:
Zip:
Insurance Carrier:
Preparer’s Name:
Law Firm:
Preparer’s Phone #:
A claim for workers’ compensation benefits is made based on the following grounds: Date of Injury or Illness: ____________
Injury Illness Repetitive Trauma Occupational Disease Physical Brain Injury Concurrent Jurisdiction
1.
2.
The claimant sustained an injury to _________________________________ (Part(s) of Body Injured) on ________________ (Month/Day/Year) in
___________ county, state of _______. Body part(s) affected are: ____________________________________________________________________________
Briefly describe how the accident occurred. ________________________________________________________________________________________________
3.
Both the claimant and the employer were subject to the South Carolina Workers’ Compensation Act at the time of injury.
4.
The relationship of employer and employee existed at the time of injury.
5.
At the time of the injury the claimant was performing services arising out of and in the course of employment.
6.
Notice of the accidental injury was given to the Employer on ____________ (Month/Day/Year) in the following manner:
____________________________________________________________________________________________________________________________________
7.
Due to injury, the claimant is in need of (check one):
(a) medical examination and treatment for: _____________________________________________________________________________________________
(b) additional medical examination and treatment for: ____________________________________________________________________________________
8.
Due to injury, the claimant requests temporary total disability benefits because of lost compensable time from work and wages for the period of:
9.
Due to the injury, the Claimant has permanent disability of the following nature and extent (check one):
(1) General Disability:
Total Partial
(2) Specific Disability:
Total Partial (3) Wage Loss
9a.
A determination of permanent disability is premature at this time.
10.
Due to the injury, the Claimant has a serious bodily disfigurement consisting of:
10a.
At the time of the injury, the Claimant was paid weekly wages of $_________, and demands accounting of days worked and wages earned as provided by law.
10b.
Give names and addresses of all employers for whom the Claimant has worked since the date of the accident:
11.
Further grounds or unusual aspects of claim:
11a.
List names and addresses of all physicians or other medical specialists who have seen or treated the Claimant as a result of the accident:
11b.
To the best of your knowledge, did you have any prior permanent disability?
If yes, describe:
12.
Appropriate benefits as provided in the Act for the above grounds and other relief as the Workers’ Compensation Commission may direct as just and proper.
13a.
I am filing a claim. I am not requesting a hearing at this time.
14.
Estimated time needed for hearing: _____________
13b.
I am requesting a hearing. A $25 fee is required.
Mediation
a. Mediation is requested to be ordered pursuant to Reg. 67-1801 B.
b. Mediation is required pursuant to Reg. 67-1802.
c. Mediation is requested by consent of the Parties pursuant to Reg. 67-1803.
d. Mediation has been conducted by a duly qualified mediator and resulted in an impasse.
Questions regarding mediation may be submitted to mediation@wcc.sc.gov.
I certify I have served this document pursuant to Reg. 67-211 by delivering a copy to______________________________________ _
address_____________________________ on the _______day of ___________20____,by first class postage certified mail personal service.
I verify the contents of this form are accurate and true to the best of my knowledge.
__________________________________ ______________________ __________________________ ____________________
Preparer’s Signature
Title
Email
Date
Questions about the use of this form should be directed to the Claims Department at 803.737.5723. Refer to Regulations 67-204 through 67-211 and Regulations
67-601 through 67-615 as well as Reg. 67-1801.
WCC Form # 50
Revised 7/13
50
Employee’s Notice of Claim and/or
Request for Hearing


