
Fillable Printable Foreign Allowances Application, Grant And Report (Sf-1190)
Fillable Printable Foreign Allowances Application, Grant And Report (Sf-1190)
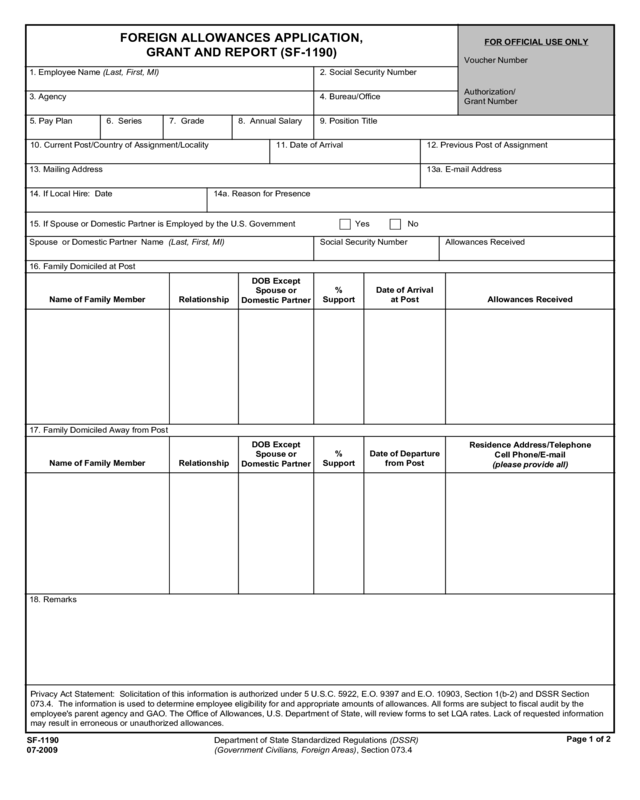
Foreign Allowances Application, Grant And Report (Sf-1190)
FOREIGN ALLOWANCES APPLICATION,
GRANT AND REPORT (SF-1190)
12. Previous Post of Assignment
9. Position Title
Name of Family Member Relationship
%
Support
Residence Address/Telephone
Cell Phone/E-mail
(please provide all)
Spouse or Domestic Partner Name (Last, First, MI)
2. Social Security Number
Department of State Standardized Regulations (DSSR)
(Government Civilians, Foreign Areas), Section 073.4
15. If Spouse or Domestic Partner is Employed by the U.S. Government
3. Agency
1. Employee Name (Last, First, MI)
4. Bureau/Office
8. Annual Salary
10. Current Post/Country of Assignment/Locality 11. Date of Arrival
13. Mailing Address
14. If Local Hire: Date
16. Family Domiciled at Post
Name of Family Member Relationship
DOB Except
Spouse or
Domestic Partner
%
Support
Date of Arrival
at Post Allowances Received
17. Family Domiciled Away from Post
Privacy Act Statement: Solicitation of this information is authorized under 5 U.S.C. 5922, E.O. 9397 and E.O. 10903, Section 1(b-2) and DSSR Section
073.4. The information is used to determine employee eligibility for and appropriate amounts of allowances. All forms are subject to fiscal audit by the
employee's parent agency and GAO. The Office of Allowances, U.S. Department of State, will review forms to set LQA rates. Lack of requested information
may result in erroneous or unauthorized allowances.
Page 1 of 2
SF-1190
07-2009
18. Remarks
6. Series 7. Grade
FOR OFFICIAL USE ONLY
Voucher Number
Authorization/
Grant Number
13a. E-mail Address
14a. Reason for Presence
Yes No
Social Security Number Allowances Received
5. Pay Plan
DOB Except
Spouse or
Domestic Partner
Date of Departure
from Post
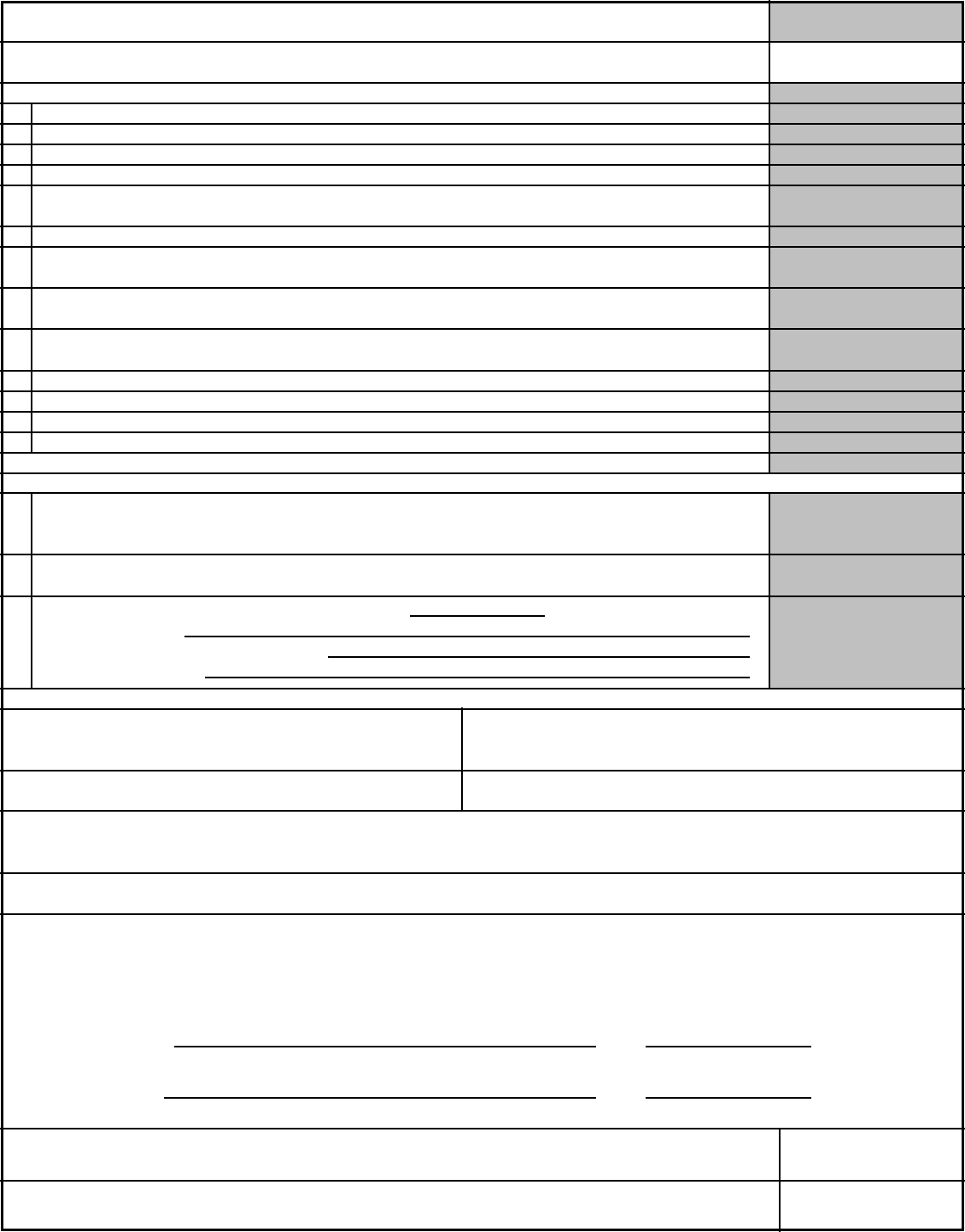
LQA (DSSR 130)
26. Certifying Official: The Above Request is Certified as Correct and Proper for Payment
24. Employee Statement and Signature: The information given on this application is true and correct to the best of my knowledge and belief. I also understand
that I am obligated to notify the authorizing office immediately of any change in conditions which may affect the amount of allowances and/or differential
authorized herein. I also understand that false statements made to the United States on this form may subject me to criminal penalties (including fines and
imprisonment) under 18 U.S.C. 287 and 1001 and/or civil penalties under 31 U.S.C. 3729 or administrative penalties under 31 U.S.C. 3802. I understand if
my employment is terminated prior to liquidation of any of these advances, any outstanding amount is due and payable immediately.
21a. Payments [Check box(es). For calculations see DSSR chapter exhibits.]
19. Employee Name (Last, First, MI)
Date
FOREIGN ALLOWANCES APPLICATION, GRANT AND REPORT
FOR OFFICIAL USE ONLY
TQSA - Temporary Quarters Subsistence Allowance - (DSSR 120)
SMA - Separate Maintenance Allowance - (DSSR 260)
TSMA - Transitional Separate Maintenance Allowance (DSSR 260)
PD - Post (Hardship) Differential (DSSR 500)
SND - Service Need Differential (Difficult to Staff Incentive Differential) (DSSR 1000)
DP - Danger Pay (DSSR 650)
PA - Post Allowance - (DSSR 220)
22a. If Electronic Funds Transfer (EFT) Mark one:
Biweekly
Advanced
Repair Allowance (DSSR 137)LQA - Living Quarters Allowance (DSSR 130)
21b. Advances
Total Amount Claimed
Beg. Date
End Date Number of Months
U.S. Dollar Payment Foreign Currency Payment
Transfer Allowance: Foreign (DSSR 240) or Home Service (DSSR 250)
Portion(s): Subsistence Miscellaneous Wardrobe Lease Penalty
Advance of Pay (DSSR 850) This advance will be repaid in
pay periods.
Travel Authorization or
Permanent Change of Station (PCS) Number
Name of Issuing Authority
Checking Savings
Financial Institution Name Financial Institution Mailing Address
Routing Number
Account Number (including any suffix)
23. Accounting Classification(s)
25. Approving/Reviewing Official Signature When Required
22b. If Paid by Check - Mailing Address, City, State, ZIP Code
Authorized Certifying Official's Signature
20. Social Security No.
End Date
End Date
End Date
Beg. Date
Beg. Date
Beg. Date
EQA - Extraordinary Quarters Allowance (DSSR 138)
Transfer Allowance: Foreign (DSSR 240) or Home Service (DSSR 250)
Lease Penalty
Voluntary Involuntary
Portion(s): Subsistence Miscellaneous Wardrobe
Education Allowance (DSSR 270)
or Travel (DSSR 280)
or 652g
Lump Sum (upon completion)
[ ]
Page 2 of 2
SF-1190
07-2009
Employee's Signature:
(If Applying for SMA on Behalf of Spouse or Domestic Partner)
Date
Spouse's or Domestic
Partner's Signature:
Voucher Number
[ ]
[ ]
[ ] [ ]
[ ] [ ] [ ] [ ]
262.3a 262.3b 262.3c 262.3d 262.3e
[ ] [ ]
[ ] [ ] [ ] [ ] [ ]
[ ] [ ]
[ ] [ ]
[ ] [ ]
[ ] [ ] [ ] [ ]
[ ] [ ]
Date
Date
0.00


