
Fillable Printable Form 245-056-000
Fillable Printable Form 245-056-000
Form 245-056-000
Department of Labor and Industries
Send original to insurer. See list on back.
Interpreter: Keep a copy for your records.
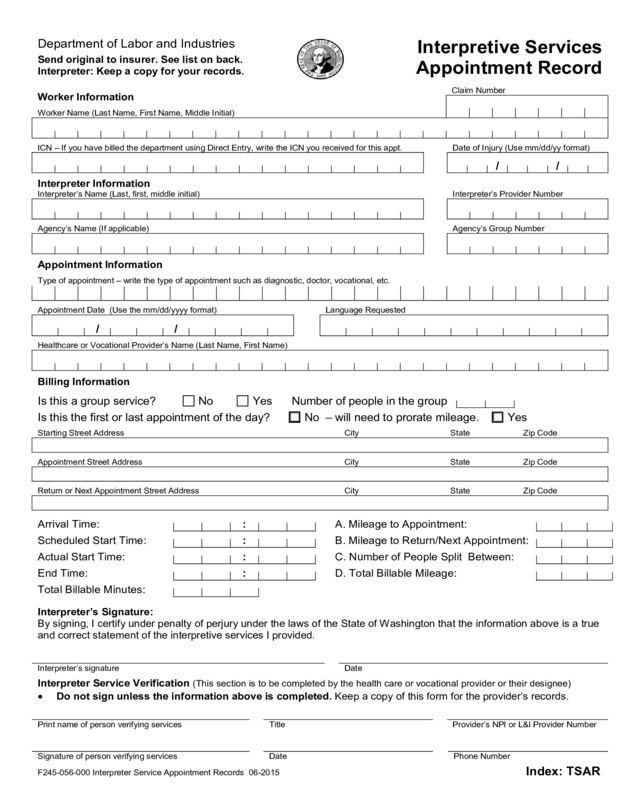
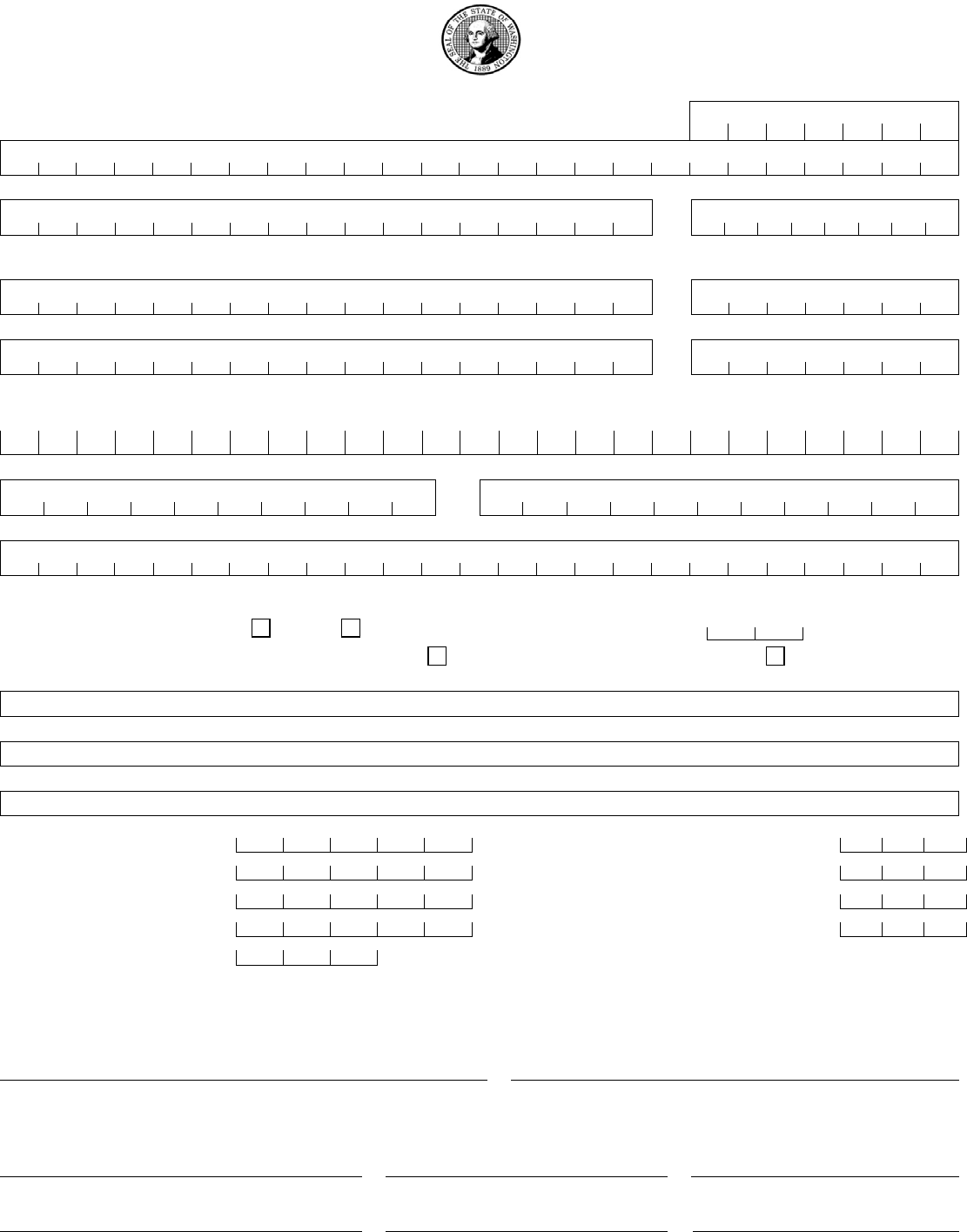
Interpretive Services
Appointment Record
Worker Information
Claim Number
Worker Name (Last Name, First Name, Middle Initial)
ICN – If you have billed the department using Direct Entry, write the ICN you received for this appt.
Date of Injury (Use mm/dd/yy format)
/
/
Interpreter Information
Interpreter’s Name (Last, first, middle initial)
Interpreter’s Provider Number
Agency’s Name (If applicable)
Agency’s Group Number
Appointment Information
Type of appointment – write the type of appointment such as diagnostic, doctor, vocational, etc.
Appointment Date (Use the mm/dd/yyyy format)
Language Requested
/
/
Healthcare or Vocational Provider’s Name (Last Name, First Name)
Billing Information
Is this a group service?
No
Yes
Number of people in the group
Is this the first or last appointment of the day?
No – will need to prorate mileage.
Yes
Starting Street Address
City
State
Zip Code
Appointment Street Address
City
State
Zip Code
Return or Next Appointment Street Address
City
State
Zip Code
Arrival Time:
:
A. Mileage to Appointment:
Scheduled Start Time:
:
B. Mileage to Return/Next Appointment:
Actual Start Time:
:
C. Number of People Split Between:
End Time:
:
D. Total Billable Mileage:
Total Billable Minutes:
Interpreter’s Signature:
By signing, I certify under penalty of perjury under the laws of the State of Washington that the information above is a true
and correct statement of the interpretive services I provided.
Interpreter’s signature
Date
Interpreter Service Verification (This section is to be completed by the health care or vocational provider or their designee)
• Do not sign unless the information above is completed. Keep a copy of this form for the provider’s records.
Print name of person verifying services
Title
Provider’s NPI or L&I Provider Number
Signature of person verifying services
Date
Phone Number
F245-056-000 Interpreter Service Appointment Records 06-2015 Index: TSAR
RESET
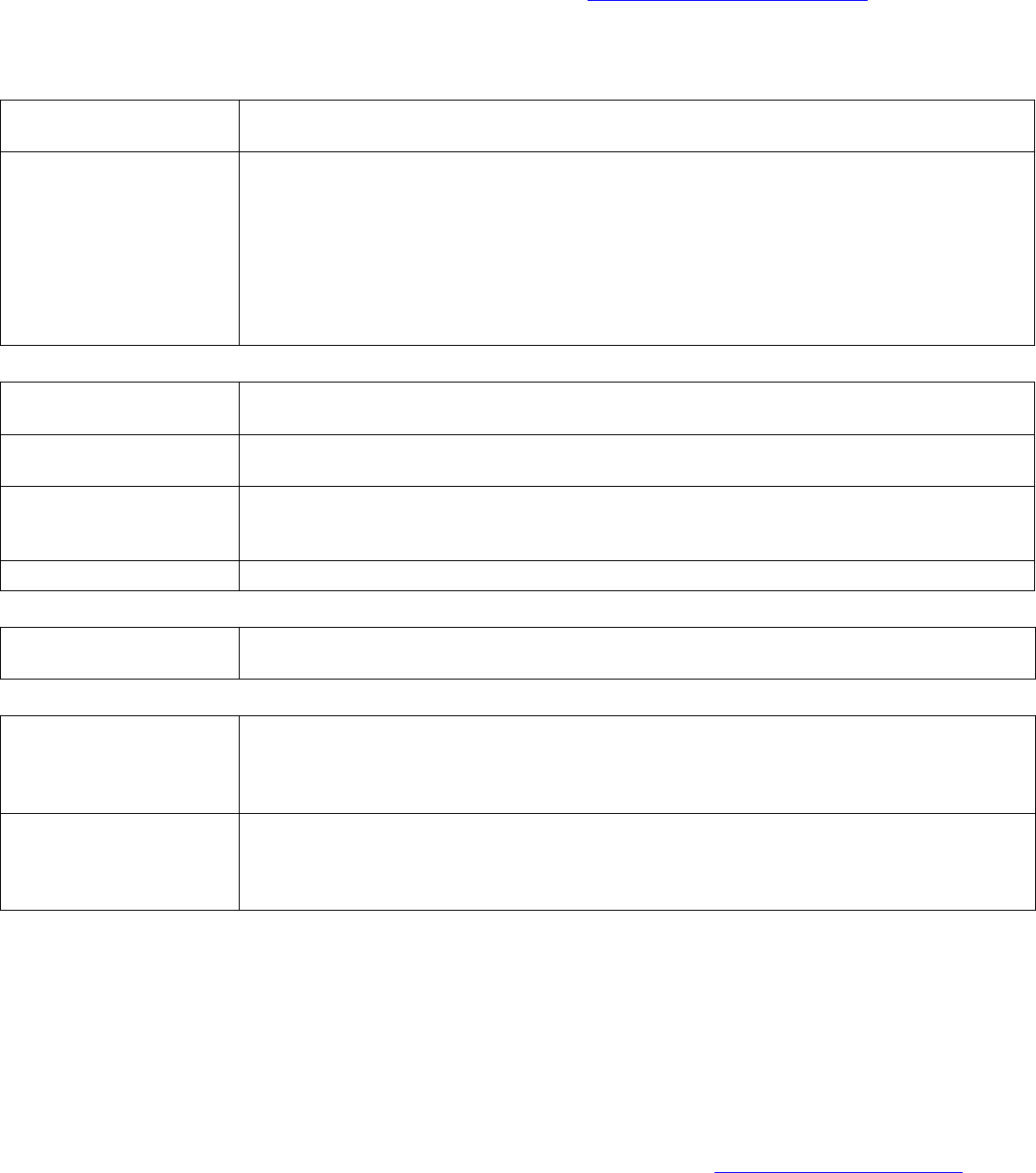
Instructions for completing Interpretive Services Appointment Record
• A completed ISAR and mileage documentation must be in the claim file by the time your bill is
processed to avoid bill denial.
• Complete billing rules and instructions can be found online at: www.Lni.wa.gov/FeeSchedules/ in the Fee
Schedules and Payment Policies (MARFS) – Chapter 14 Interpretive Services
Complete the entire form. See below for detailed information on our most questioned fields.
Worker Information:
Worker Name
Enter the worker name in the last name, first name, middle initial format. If there aren’t
enough spaces for the entire worker name, enter as much of the name as possible.
ICN If you bill for interpretive services using L&I’s Provider Express Billing (PEB) Direct
Entry, enter the internal control number (ICN) assigned to the bill you submitted. The
ICN assigned to your bill can be found in the Adjust Direct Entry Bills function of PEB for
the claim number and date of service (DOS) billed.
Please note – ICNs are only immediately available during PEB’s normal operating hours
of Monday – Friday, 6:00 am to 6:00 pm, excluding state holidays. If you submit your bill
outside of normal operating hours, your ICN won’t be available until normal operating
hours.
Interpreter Information:
Interpreter’s Name
Enter the name of the person who provided the interpretation services. If there aren’t
enough spaces for the entire interpreter’s name, enter as much of the name as possible.
Interpreter’s Provider
Number
Enter the L&I provider payment number assigned to the interpreter who provided the
interpretation services.
Agency’s Name If the interpreter provided services on behalf of an interpretation agency, write the
agency’s name. If there aren’t enough spaces for the entire agency name, enter as
much of the name as possible.
Agency’s Group Number
Enter the L&I provider payment number assigned to the interpretation agency.
Appointment Information:
Type of Appointment
Write the type of appointment for provided interpretive services, such as doctor,
diagnostic, vocational, etc.
Billing Information:
Group Service
If this is for a group service, check the “Yes” box. In the space provided, write the
number of people in the group. Group service time must be divided between ALL clients
in the group. For more information, please refer to the Fee Schedules and Payment
Policies (MARFS) – Chapter 14 Interpretive Services (see the link above).
First or Last
Appointment of the Day
Check the appropriate box. If this is not the first or last appointment of the day, you will
need to split the mileage between the L&I client and the next client – regardless of who
the next client is. For more information, please refer to the Fee Schedules and Payment
Policies (MARFS) – Chapter 14 Interpretive Services (see the link above).
How to submit your bill: Mail your bill or use our Direct Entry Billing. Do not fax your bill.
How to submit your ISAR: Submit the original to the insurer. Use addresses and fax numbers below only for the
ISAR and mileage documentation.
State Fund
Department of Labor and Industries
PO Box 44291
Olympia WA 98504-4291
800-848-0811 or 360-902-6500
Fax: 360-902-4567
Crime Victims Compensation
Department of Labor and Industries
PO Box 44520
Olympia WA 98504-4520
800-762-3716 or 360-902-5377
Fax: 360-902-5333
Self-Insurer
Varies – Call 360-902-6901 to
obtain the insurer’s phone number
and address
Or see the Self-Insurer list:
www.Lni.wa.gov/SelfInsured
F245-056-000 Interpreter Service Appointment Records 06-2015 Index: TSAR


