
Fillable Printable Form 245-346-000
Fillable Printable Form 245-346-000
Form 245-346-000
F245-346-000 job modification assistance application p1 12-2008 Index:
JMOD
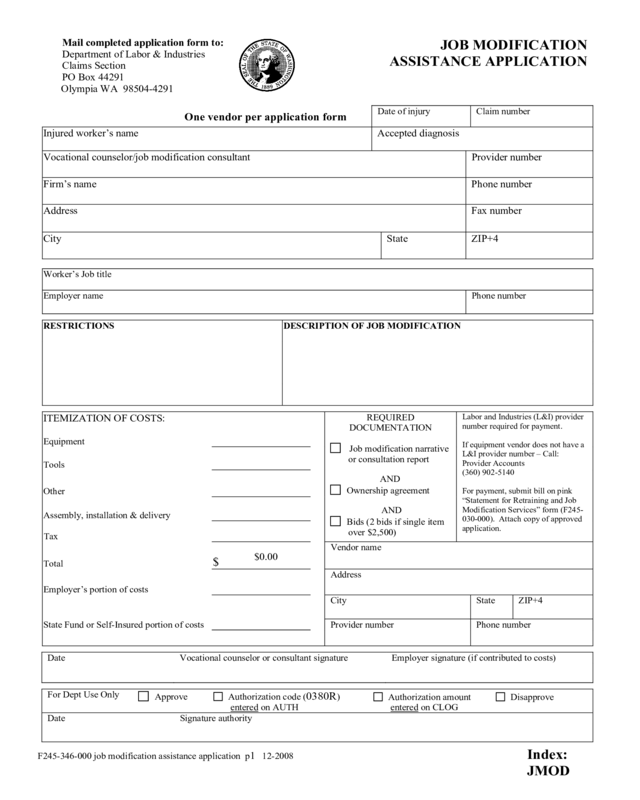
Mail completed application form to:
Department of Labor & Industries
Claims Section
PO Box 44291
Olympia WA 98504-4291
JOB MODIFICATION
ASSISTANCE APPLICATION
One vendor per application form
Date of injury
Claim number
Injured worker’s name
Accepted diagnosis
Vocational counselor/job modification consultant Provider number
Firm’s name
Phone number
Address
Fax number
City
State
ZIP+4
Worker’s Job title
Employer name
Phone number
RESTRICTIONS
DESCRIPTION OF JOB MODIFICATION
ITEMIZATION OF COSTS:
REQUIRED
DOCUMENTATION
Job modification narrative
or consultation report
AND
Ownership agreement
AND
Bids (2 bids if single item
over $2,500)
Labor and Industries (L&I) provider
number required for payment.
If equipment vendor does not have a
L&I provider number – Call:
Provider Accounts
(360) 902-5140
For payment, submit bill on pink
“Statement for Retraining and Job
Modification Services” form (F245-
030-000). Attach copy of approved
application.
Equipment
Tools
Other
Assembly, installation & delivery
Tax
Total
$
Vendor name
Employer’s portion of costs
Address
State Fund or Self-Insured portion of costs
City State ZIP+4
Provider number Phone number
Date Vocational counselor or consultant signature Employer signature (if contributed to costs)
For Dept Use Only
Approve
Authorization code (0380R)
entered on AUTH
Authorization amount
entered
on CLOG
Disapprove
Date Signature authority
$0.00
F245-346-000 job modification assistance application p2 12-2008 Index:
JMOD
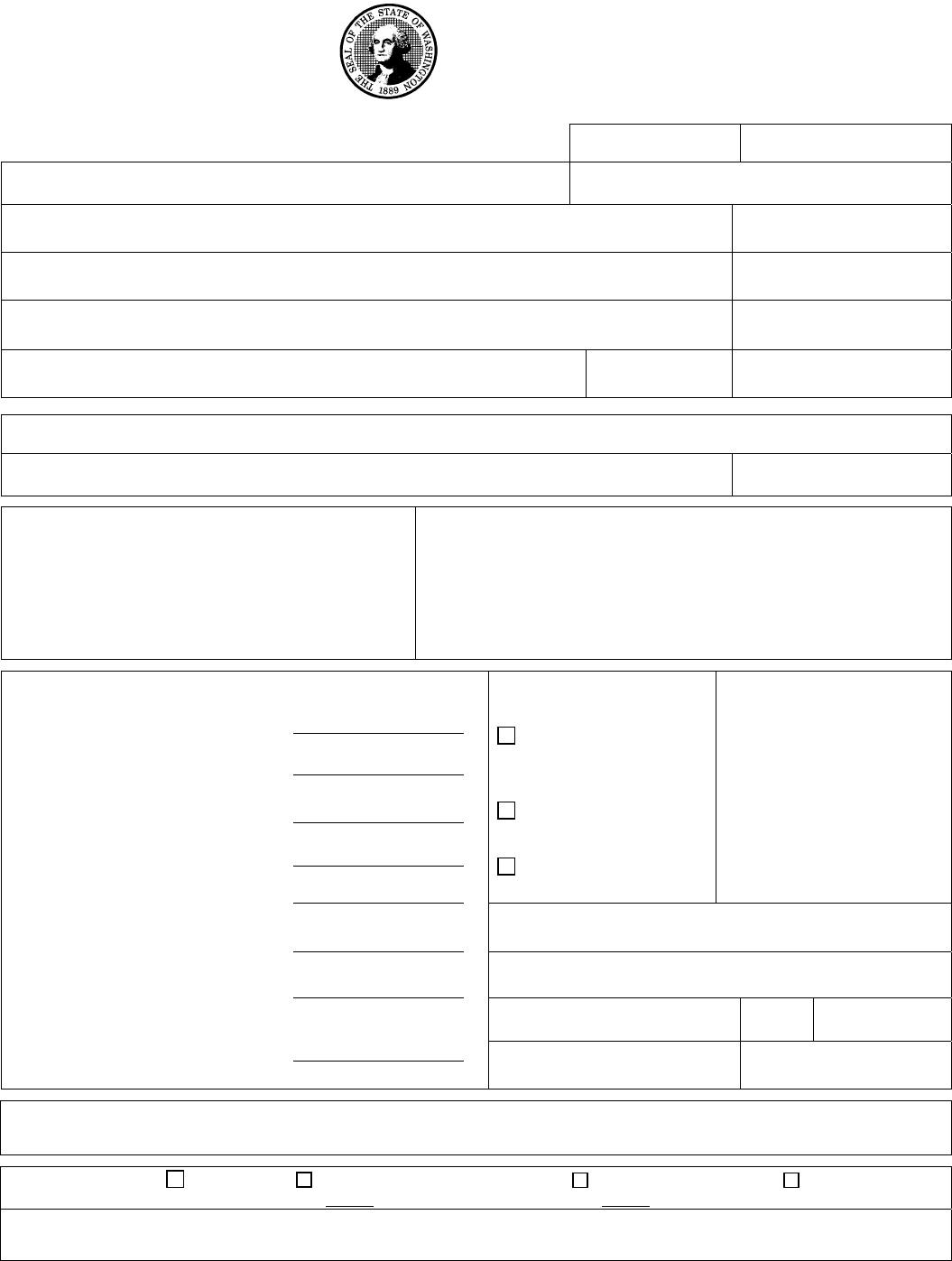
Ownership Agreement for Tools and Equipment
Purchased as a Job Modification
Worker: ____________________________ Claim #: ____________________________
Employer:___________________________
This modification is being provided to accommodate my work restrictions so I may perform my job duties and
return to work.
My employer and I will need to agree upon who will own the equipment and note it below. (Typically, a
worker would be listed as the owner for any portable items.)
The designated party will own these items when I successfully return to work. Any equipment owned by the
employer must remain available to me during my shift.
Maintenance Responsibility:
Safekeeping, proper maintenance and repair of the equipment (beyond the expiration of the manufacturer’s
warranty, if applicable) are the responsibility of the identified owner.
Return Policy:
I will return any items to L&I if not used by me or if I am not able to successfully return to work. I will contact
L&I and make arrangements to return the equipment to the nearest service location.
If the employer paid for any cost of the modification, or the equipment is affixed to the work site, the employer
may retain the equipment, regardless of the outcome of the modification or return to work.
I understand the agreement above and I am willing to comply with the terms.
______________________________________________ __________________
Worker Signature Date
______________________________________________ __________________
Employer Signature Date
Inventory
Equipment/model # Owner (upon successful completion)
RESET

F245-346-000 job modification assistance application p3 12-2008 Index:
JMOD
INSTRUCTIONS FOR COMPLETING THE JOB MODIFICATION ASSISTANCE APPLICATION FORM
(F245-346-000)
NOTE: SUBMIT A SEPARATE APPLICATION FOR EACH VENDOR.
1) DATE OF INJURY: Record the date of injury.
2) CLAIM NUMBER: For the injured worker on whose behalf the application is being submitted.
3) INJURED WORKER’S NAME: Injured worker’s full name.
4) ACCEPTED DIAGNOSIS: Record the accepted industrial condition(s).
5) VOCATIONAL COUNSELOR/JOB MODIFICATION CONSULTANT: Record the name of the individual submitting
the application (must be vocational counselor, job modification consultant, or employer that has been trained in
completing the applications.) May not be submitted by the worker.
a) FIRM NAME: Record the firm that the vocational counselor/job modification consultant represents.
b) PROVIDER NO.: Record the vocational counselor/job modification consultant’s provider number.
c) ADDRESS: Record the vocational counselor/job modification consultant’s address, phone, and fax number.
6) JOB TITLE: Record the actual or anticipated job title for which the application is being submitted.
7) EMPLOYER NAME: Record the employer’s name and telephone number for the job title listed.
8) DESCRIPTION OF WORK RESTRICTIONS: List the restrictions or limitations in physical capacities that relate to the
requested modification.
9) DESCRIPTION OF JOB MODIFICATION: Briefly list the equipment being requested and the reason for the request.
10) ITEMIZATION OF COSTS:
a) EQUIPMENT: Record the cost of equipment being requested.
b) TOOLS: Record the cost of any tools being requested.
c) OTHER: Record the cost of non-equipment, non-tool items, such as training time.
d) ASSEMBLY: Record the cost of assembly, installation and delivery.
e) TOTAL: Record total cost of modifications requested for this vendor.
f) EMPLOYER’S PORTION: Record the amount the employer will pay to the vendor.
g) STATE FUND (SF) OR SELF-INSURED (SIE) PORTION: Record the amount the SF or SIE is asked to pay.
11) REQUIRED DOCUMENTATION
a) REPORT: If the report has been previously submitted, please indicate that it is “on file”.
b) BIDS: Submit two bids for any item over $2,500.00. The price includes any tax, shipping, delivery, and training
charges. If the item is only available from one vendor, please specify that it is a sole source item.
c) OWNERSHIP AGREEMENT: Submit completed form F245-346-000, page 2.
12) VENDOR: Enter the vendor’s name, address, phone and provider number. Vendors must have a provider number in
order to be reimbursed.


