
Fillable Printable Form 4732 - Missouri Department Of Revenue
Fillable Printable Form 4732 - Missouri Department Of Revenue
Form 4732 - Missouri Department Of Revenue
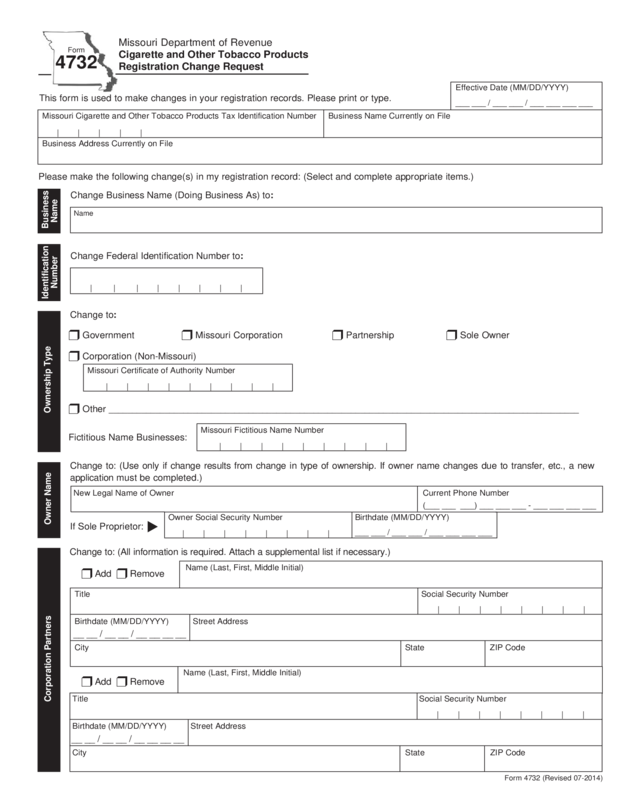
Change to: (Use only if change results from change in type of ownership. If owner name changes due to transfer, etc., a new
application must be completed.)
If Sole Proprietor:
Fictitious Name Businesses:
Missouri Department of Revenue
Cigarette and Other Tobacco Products
Registration Change Request
Form
4732
This form is used to make changes in your registration records. Please print or type.
Missouri Cigarette and Other Tobacco Products Tax Identification Number Business Name Currently on File
Business Address Currently on File
Please make the following change(s) in my registration record: (Select and complete appropriate items.)
Change to: (All information is required. Attach a supplemental list if necessary.)
Form 4732 (Revised 07-2014)
| | | | |
Ownership Type
Change Business Name (Doing Business As) to:
Name
Business
Name
t
Owner Name
Owner Social Security Number
| | | | | | | |
Birthdate (MM/DD/YYYY)
___ ___ / ___ ___ / ___ ___ ___ ___
New Legal Name of Owner Current Phone Number
Corporation Partners
Name (Last, First, Middle Initial)
Title Social Security Number
Birthdate (MM/DD/YYYY) Street Address
City State ZIP Code
| | | | | | | |
r Add r Remove
__ __ / __ __ / __ __ __ __
r Add r Remove
Name (Last, First, Middle Initial)
Title Social Security Number
Birthdate (MM/DD/YYYY) Street Address
City State ZIP Code
| | | | | | | |
__ __ / __ __ / __ __ __ __
r Government r Missouri Corporation r Partnership r Sole Owner
r Corporation (Non-Missouri)
r Other _____________________________________________________________________________________________________
Missouri Certificate of Authority Number
| | | | | | | | |
Change Federal Identification Number to:
Identification
Number
Change to:
(___ ___ ___) ___ ___ ___ - ___ ___ ___ ___
| | | | | | | |
| | | | | | | | |
Missouri Fictitious Name Number
Effective Date (MM/DD/YYYY)
___ ___ / ___ ___ / ___ ___ ___ ___
Reset Form
Print Form
Form 4732 (Revised 07-2014)
Mail to: Taxation Division Phone: (573) 751-7163
P.O. Box 811 Fax: (573) 522-1720
Jefferson City, MO 65105-0811 TTY: (800) 735-2966
Visit http://www.dor.mo.gov/business/tobacco/ for additional information.
Change Address to:
r Physical Address r Mailing Address r Location of Books and Records
r Attach original rider from bonding company covering change of name or physical address
r A new bond indicating change of ownership accompanied by new application
Street Address City State ZIP Code County
Address
AttachmentsSignature
Signature Printed Name
Title Date (MM/DD/YYYY)
Under penalties of perjury, I declare that the above information and any attached supplement is true, completed, and correct.
__ __ /__ __ /__ __ __ __


