
Fillable Printable Form 4854 - Employer Withholding Tax Refund Request
Fillable Printable Form 4854 - Employer Withholding Tax Refund Request
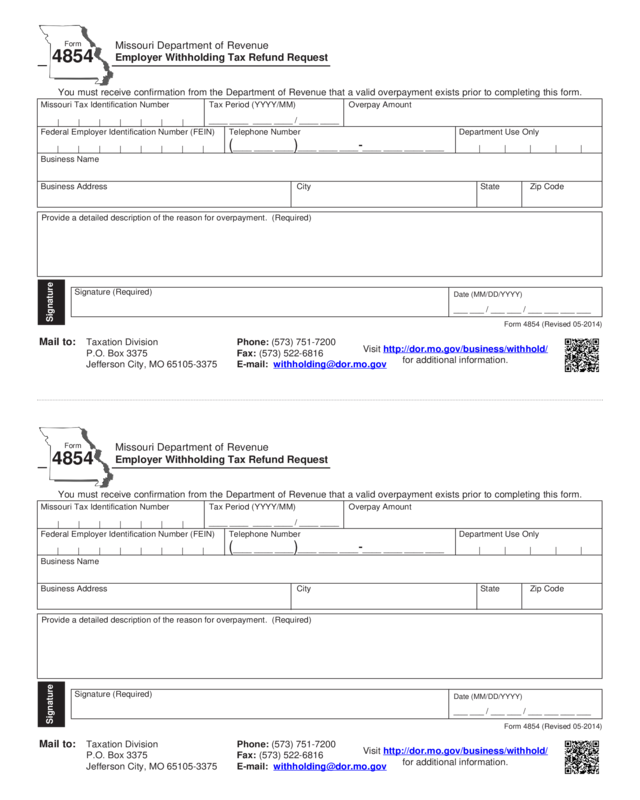
Form 4854 - Employer Withholding Tax Refund Request
Missouri Tax Identification Number Tax Period (YYYY/MM) Overpay Amount
Federal Employer Identification Number (FEIN) Telephone Number Department Use Only
Business Name
Business Address City State Zip Code
(____ ____ ____)____ ____ ____-____ ____ ____ ____
Missouri Department of Revenue
Employer Withholding Tax Refund Request
Form
4854
Form 4854 (Revised 05-2014)
You must receive confirmation from the Department of Revenue that a valid overpayment exists prior to completing this form.
Signature (Required)
Signature
Date (MM/DD/YYYY)
___ ___ / ___ ___ / ___ ___ ___ ___
Mail to: Taxation Division Phone: (573) 751-7200
P.O. Box 3375 Fax: (573) 522-6816
Visit http://dor.mo.gov/business/withhold/
for additional information.
Provide a detailed description of the reason for overpayment. (Required)
| | | | | | |
| | | | | | | |
____ ____ ____ ____ / ____ ____
| | | | |
Missouri Tax Identification Number Tax Period (YYYY/MM) Overpay Amount
Federal Employer Identification Number (FEIN) Telephone Number Department Use Only
Business Name
Business Address City State Zip Code
(____ ____ ____)____ ____ ____-____ ____ ____ ____
Missouri Department of Revenue
Employer Withholding Tax Refund Request
Form
4854
Form 4854 (Revised 05-2014)
You must receive confirmation from the Department of Revenue that a valid overpayment exists prior to completing this form.
Signature (Required)
Signature
Date (MM/DD/YYYY)
___ ___ / ___ ___ / ___ ___ ___ ___
Mail to: Taxation Division Phone: (573) 751-7200
P.O. Box 3375 Fax: (573) 522-6816
Visit http://dor.mo.gov/business/withhold/
for additional information.
Provide a detailed description of the reason for overpayment. (Required)
| | | | | | |
| | | | | | | |
____ ____ ____ ____ / ____ ____
| | | | |
Reset Form
Print Form


