
- Form DPR-125 - Drinking Driver Program Classroom Site Inspection Report - New York
- Form DPR-102 - Drinking Driver Program Instructor Application - New York
- Form MV-15MOU - Understanding Memorandum (Driver Privacy Protection Act) - New York
- Form MV-1W - Withdrawal of Consent - New York
- Form DPR-152 - Drinking Driver Program Annual Enrollment Report - New York
- Form DPR-151 - DDP Fiscal Report - New York
Fillable Printable Form DS-451 - Consent for Release of Information - New York
Fillable Printable Form DS-451 - Consent for Release of Information - New York
Form DS-451 - Consent for Release of Information - New York
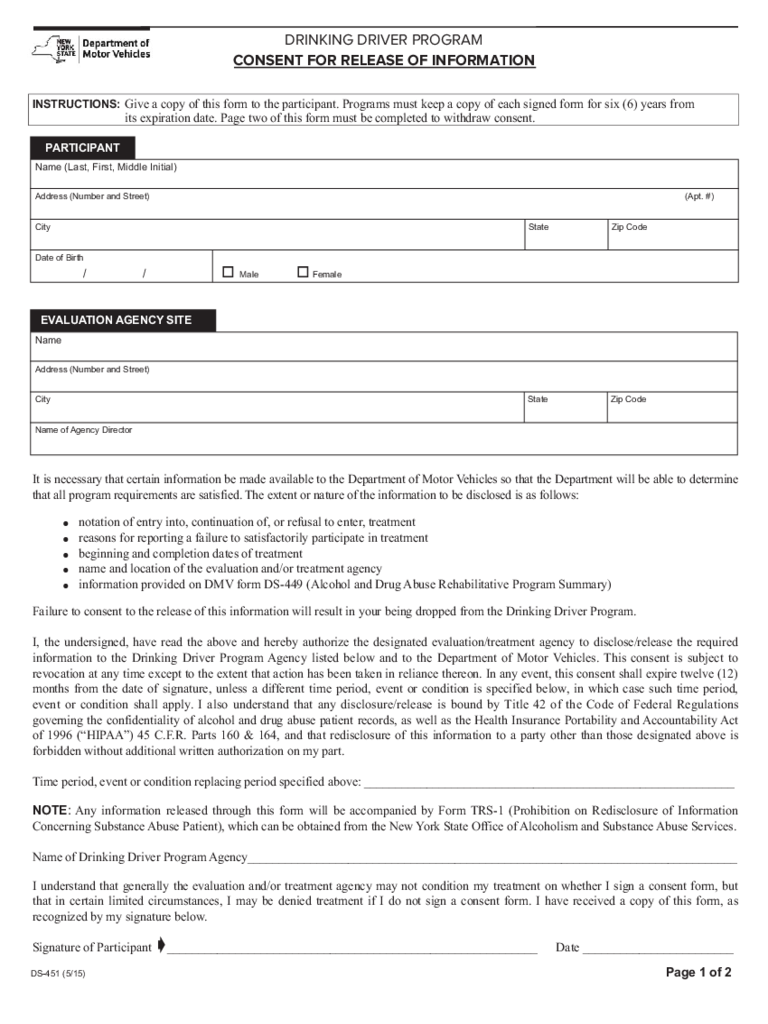
DRINKING DRIVER PROGRAM
CONSENT FOR RELEASE OF INFORMATION
It is necessary that certain information be made available to the Department of Motor Vehicles so that the Department will be able to determine
that all program requirements are satisfied. The extent or nature of the information to be disclosed is as follows:
l notation of entry into, continuation of, or refusal to enter, treatment
l reasons for reporting a failure to satisfactorily participate in treatment
l beginning and completion dates of treatment
l name and location of the evaluation and/or treatment agency
l information provided on DMV form DS-449 (Alcohol and Drug Abuse Rehabilitative Program Summary)
Failure to consent to the release of this information will result in your being dropped from the Drinking Driver Program.
I, the undersigned, have read the above and hereby authorize the designated evaluation/treatment agency to disclose/release the required
information to the Drinking Driver Program Agency listed below and to the Department of Motor Vehicles. This consent is subject to
revocation at any time except to the extent that action has been taken in reliance thereon. In any event, this consent shall expire twelve (12)
months from the date of signature, unless a different time period, event or condition is specified below, in which case such time period,
event or condition shall apply. I also understand that any disclosure/release is bound by Title 42 of the Code of Federal Regulations
governing the confidentiality of alcohol and drug abuse patient records, as well as the Health Insurance Portability and Accountability Act
of 1996 (“HIPAA”) 45 C.F.R. Parts 160 & 164, and that redisclosure of this information to a party other than those designated above is
forbidden without additional written authorization on my part.
Time period, event or condition replacing period specified above: ___________________________________________________________
NOTE: Any information released through this form will be accompanied by Form TRS-1 (Prohibition on Redisclosure of Information
Concerning Substance Abuse Patient), which can be obtained from the New York State Office of Alcoholism and Substance Abuse Services.
Name of Drinking Driver Program Agency______________________________________________________________________________
I understand that generally the evaluation and/or treatment agency may not condition my treatment on whether I sign a consent form, but
that in certain limited circumstances, I may be denied treatment if I do not sign a consent form. I have received a copy of this form, as
recognized by my signature below.
Signature of Participant __________________________________________ _________________ Date ________________________
PARTICIPANT
Name (Last, First, Middle Initial)
Address (Number and Street)
(Apt. #)
City
Date of Birth
/ /
o Male o Female
State Zip Code
EVALUATION AGENCY SITE
Name
Address (Number and Street)
City
Name of Agency Director
State Zip Code
ç
DS-451 (5/15)
Page 1 of 2
Give a copy of this form to the participant. Programs must keep a copy of each signed form for six (6) years from
its expiration date. Page two of this form must be completed to withdraw consent.
INSTRUCTIONS:
DRINKING DRIVER PROGRAM
WITHDRAWAL OF CONSENT FOR RELEASE OF INFORMATION
DS-451 (5/15)
Page 2 of 2
Give a copy of this form to the participant. Completion of this page withdraws the consent indicated on page one.
I, the undersigned, hereby withdraw my authorization to disclose information to the above named individual(s)/organization(s), except to
the extent that action has already been taken in reliance upon it.
I understand that generally the evaluation and/or treatment agency may not condition my treatment on whether I agree to sign a consent
form, but that in certain circumstances, I may be denied treatment if I do not sign, or if I withdraw consent. I also recognize that if I
withdraw consent, it will result in me being dropped from the Drinking Driver Program. I have received a copy of this form, as recognized
by my signature below.
Name of Person or Organization to Which the Disclosure Was Authorized:
New York State Department of Motor Vehicles
(Name of Drinking Driver Program Agency)
Name of Person or Organization Disclosing Information:
(Name of Evaluation and/or Treatment Agency)
ç
(Signature of Participant)
(Print Name of Participant)
(Date)
INSTRUCTIONS:
reset/clear


