
- Form MV-80W - Application for Tinted Window Exemption - New York
- Form MV-262 - Certification of Supervised Driving - New York
- Form ID-44EDL - Proofs of Identity, U.S. Citizenship and Residency - New York
- Form MV-58A - Certificate of Employment - New York
- Form MV-TEENS - TEENS Enrollment and Consent Form - New York
- Form MV-619 - Vision Test Report - New York
Fillable Printable Form DS-6 - Physician's Request for Driver Review - New York
Fillable Printable Form DS-6 - Physician's Request for Driver Review - New York
Form DS-6 - Physician's Request for Driver Review - New York
Have you treated this patient? o YES o NO
If Yes: Date of Last Examination? _______________________.
Please describe the condition that you have treated or are currently treating:
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
Is the patient receiving medication for this condition? o YES o NO
If Yes: Please specify the type and dosage:
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
In my medical opinion, (please check one):
o the patient’s condition may affect the safe operation of a motor vehicle, and the patient should be evaluated by the Department of
Motor Vehicles
o the patient’s condition prevents the safe operation of a motor vehicle and driving privileges should be suspended.
Please provide further detail in the space provided or in an attached statement on your letterhead:
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
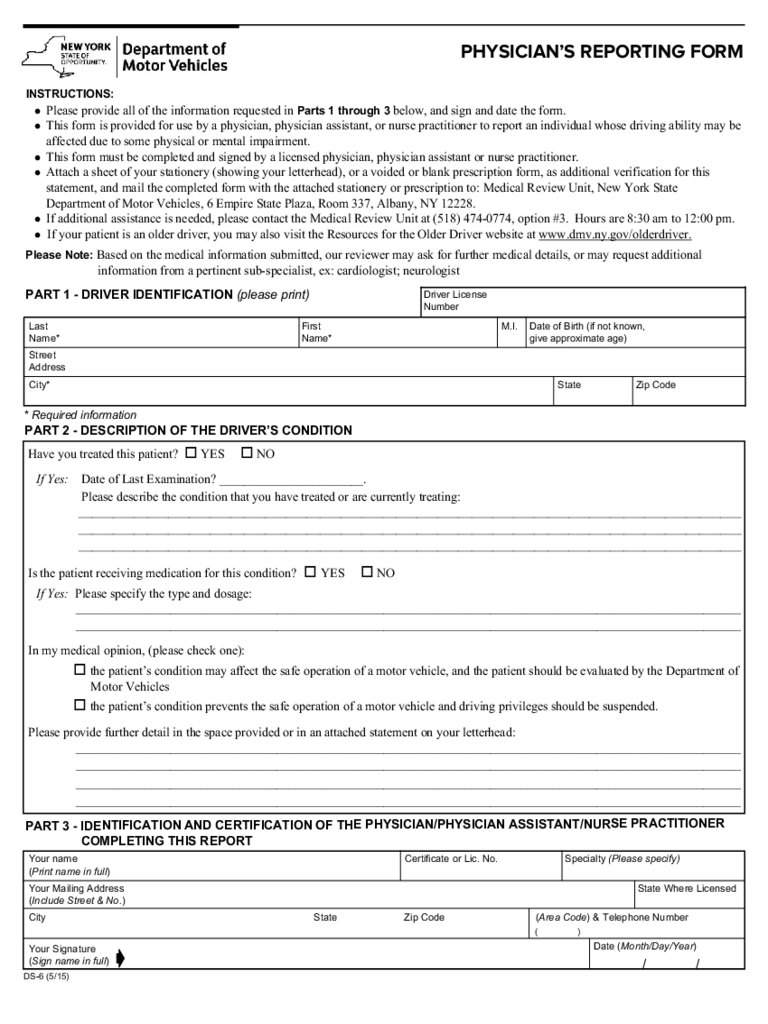
PHYSICIAN’S REPORTING FORM
INSTRUCTIONS:
l Please provide all of the information requested in Parts 1 through 3 below, and sign and date the form.
l This form is provided for use by a physician, physician assistant, or nurse practitioner to report an individual whose driving ability may be
affected due to some physical or mental impairment.
l This form must be completed and signed by a licensed physician, physician assistant or nurse practitioner.
l Attach a sheet of your stationery (showing your letterhead), or a voided or blank prescription form, as additional verification for this
statement, and mail the completed form with the attached stationery or prescription to: Medical Review Unit, New York State
Department of Motor Vehicles, 6 Empire State Plaza, Room 337, Albany, NY 12228.
l If additional assistance is needed, please contact the Medical Review Unit at (518) 474-0774, option #3. Hours are 8:30 am to 12:00 pm.
l If your patient is an older driver, you may also visit the Resources for the Older Driver website at www.dmv.ny.gov/olderdriver.
PART 1 - DRIVER IDENTIFICATION (please print)
PART 2 - DESCRIPTION OF THE DRIVER’S CONDITION
Last
Name*
Street
Address
City* State
Driver License
Number
Zip Code
First
Name*
M.I. Date of Birth (if not known,
give approximate age)
DS-6 (5/15)
* Required information
Your name
(Print name in full)
Your Mailing Address
(Include Street & No.)
Your Signature
(Sign name in full)
City
Date (Month/Day/Year)
/ /
State Zip Code
(Area Code) & Telephone Number
( )
Certificate or Lic. No.
State Where Licensed
ç
Specialty (Please specify)
PART 3 - IDENTIFICATION AND CERTIFICATION OF THE PHYSICIAN/PHYSICIAN ASSISTANT/NURSE PRACTITIONER
COMPLETING THIS REPORT
Please Note: Based on the medical information submitted, our reviewer may ask for further medical details, or may request additional
information from a pertinent sub-specialist, ex: cardiologist; neurologist
reset/clear


