
- Form IRP-21 - IRP TEAR Request Form - New York
- Form DS-3 - Article 19-A Annual Affidavit of Compliance - New York
- Form DS-872 - Carrier's Annual Review of Employee's Driving Record - New York
- Form DS-870 - Article 19-A Bus Driver Application - New York
- Form DS-874C - Supplement to: Medical Examination of Driver Report - New York
- Form DS-19 - Motor Carrier Accident and Conviction Notification Program Application - New York
Fillable Printable Form DS-703 - Article 19-A Bus Driver's Blood Pressure Follow-Up - New York
Fillable Printable Form DS-703 - Article 19-A Bus Driver's Blood Pressure Follow-Up - New York
Form DS-703 - Article 19-A Bus Driver's Blood Pressure Follow-Up - New York
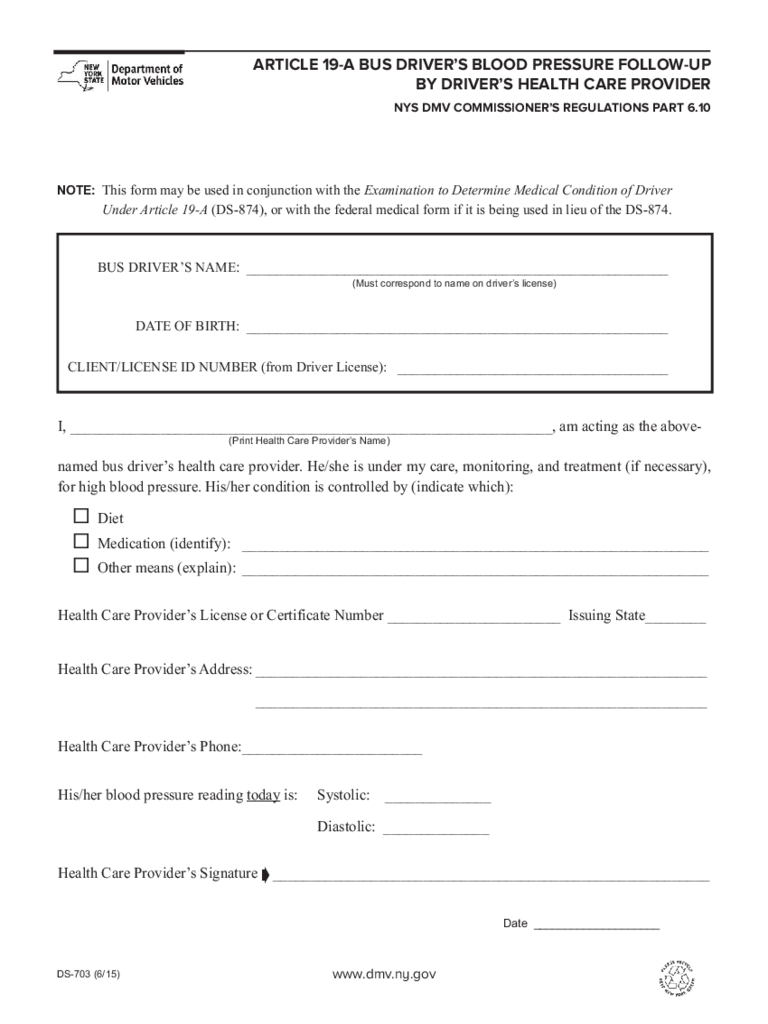
ARTICLE 19-A BUS DRIVER’S BLOOD PRESSURE FOLLOW-UP
BY DRIVER’S HEALTH CARE PROVIDER
NYS DMV COMMISSIONER’S REGULATIONS PART 6.10
I, ________________________________________________________________, am acting as the above-
named bus driver’s health care provider. He/she is under my care, monitoring, and treatment (if necessary),
for high blood pressure. His/her condition is controlled by (indicate which):
www.dmv.ny.gov
DS-703 (6/15)
(Print Health Care Provider’s Name)
¨ Diet
¨ Medication (identify): ______________________________________________________________
¨ Other means (explain): ______________________________________________________________
Health Care Provider’s License or Certificate Number _______________________ Issuing State________
Health Care Provider’s Address: ____________________________________________________________
____________________________________________________________
Health Care Provider’s Phone:________________________
His/her blood pressure reading today is: Systolic: ______________
Diastolic: ______________
Health Care Provider’s Signature __________________________________________________________
Â
BUS DRIVER’S NAME: ________________________________________________________
DATE OF BIRTH: ________________________________________________________
CLIENT/LICENSE ID NUMBER (from Driver License): ____________________________________
(Must correspond to name on driver’s license)
NOTE: This form may be used in conjunction with the Examination to Determine Medical Condition of Driver
Under Article 19-A (DS-874), or with the federal medical form if it is being used in lieu of the DS-874.
Date ____________________
reset/clear


