
- Form FS-25 - Request for Insurance Information for NY Registrants - New York
- Form DS-1 - Out-of-State Drinking/Drugged Driving Program Enrollment and Status Form - New York
- Form AA-3.3 - Application to Reopen Default Conviction - New York
- Form FS-15 - Affirmation Under Vehicle and Traffic Law - New York
- Form AA-15 - TVB Ticket Management for Attorneys Application - New York
- Form AA-33 - TVB Appeal Form - New York
Fillable Printable Form FS-15 - Affirmation Under Vehicle and Traffic Law - New York
Fillable Printable Form FS-15 - Affirmation Under Vehicle and Traffic Law - New York
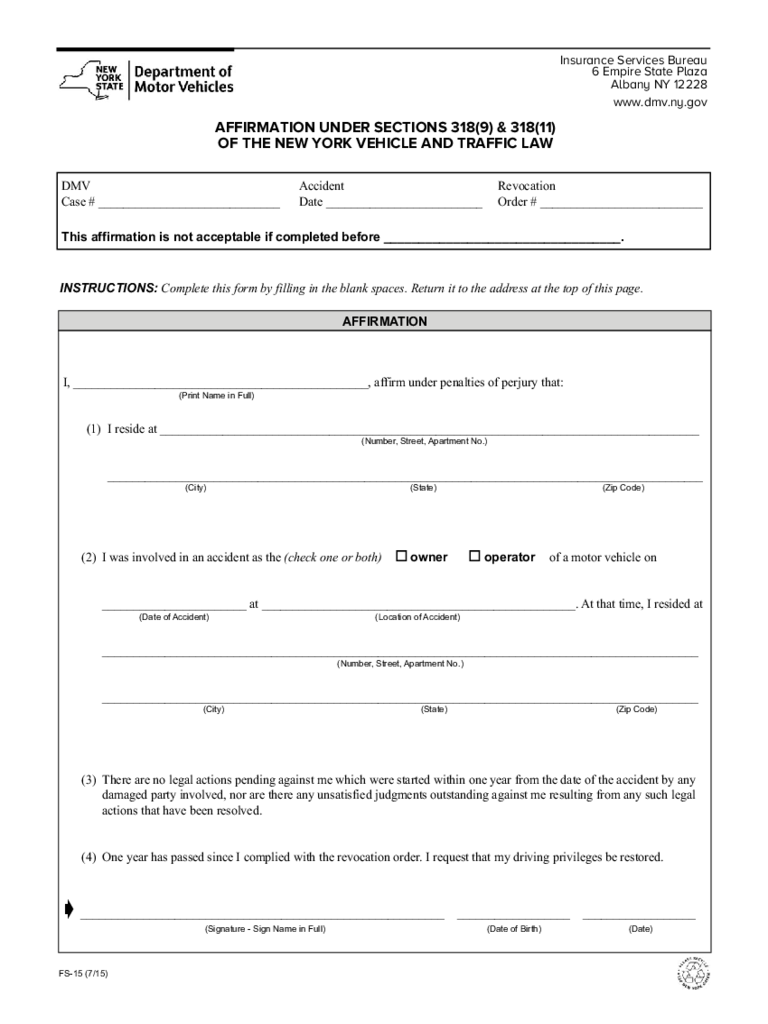
Form FS-15 - Affirmation Under Vehicle and Traffic Law - New York
Insurance Services Bureau
6 Empire State Plaza
Albany NY 12228
www.dmv.ny.gov
AFFIRMATION UNDER SECTIONS 318(9) & 318(11)
OF THE NEW YORK VEHICLE AND TRAFFIC LAW
I, _______________________________________________, affirm under penalties of perjury that:
(1) I reside at ______________________________________________________________________________________
_______________________________________________________________________________________________
(Print Name in Full)
(Number, Street, Apartment No.)
(City) (State) (Zip Code)
(2) I was involved in an accident as the (check one or both) o owner o operator of a motor vehicle on
_______________________ at __________________________________________________. At that time, I resided at
_______________________________________________________________________________________________
_______________________________________________________________________________________________
(3) There are no legal actions pending against me which were started within one year from the date of the accident by any
damaged party involved, nor are there any unsatisfied judgments outstanding against me resulting from any such legal
actions that have been resolved.
(4) One year has passed since I complied with the revocation order. I request that my driving privileges be restored.
ç __________________________________________________________ __________________ __________________
(Date of Accident)
(Number, Street, Apartment No.)
(City) (State) (Zip Code)
(Location of Accident)
(Signature - Sign Name in Full) (Date of Birth) (Date)
DMV Accident Revocation
Case # _____________________________ Date _________________________ Order # __________________________
INSTRUCTIONS: Complete this form by filling in the blank spaces. Return it to the address at the top of this page.
This affirmation is not acceptable if completed before __________________________________.
FS-15 (7/15)
AFFIRMATION


