
Fillable Printable Form Twcc-1
Fillable Printable Form Twcc-1
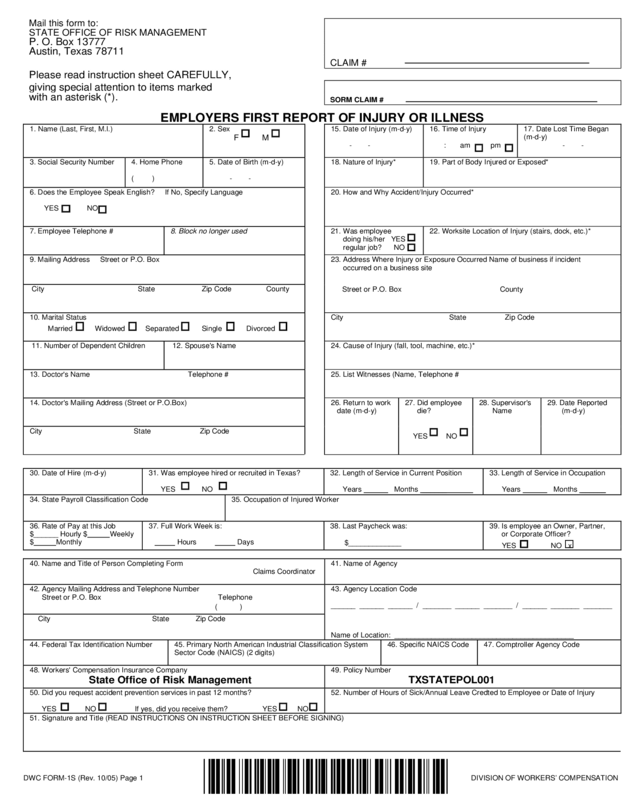
Form Twcc-1
Mail this form to:
STATE OFFICE OF RISK MANAGEMENT
P. O. Box 13777
Austin, Texas 78711
CLAIM #
Please read instruction sheet CAREFULLY,
giving special attention to items marked
with an asterisk (*).
SORM CLAIM #
EMPLOYERS FIRST REPORT OF INJURY OR ILLNESS
DWC FORM-1S (Rev. 10/05) Page 1 DIVISION OF WORKERS’ COMPENSATION
1. Name (Last, First, M.I.) 2. Sex
F M
15. Date of Injury (m-d-y)
- -
16. Time of Injury
: am pm
17. Date Lost Time Began
(m-d-y)
- -
3. Social Security Number
4. Home Phone
( )
5. Date of Birth (m-d-y)
- -
18. Nature of Injury* 19. Part of Body Injured or Exposed*
6. Does the Employee Speak English? If No, Specify Language
YES NO
20. How and Why Accident/Injury Occurred*
7. Employee Telephone #
8. Block no longer used
21. Was employee
doing his/her YES
regular job? NO
22. Worksite Location of Injury (stairs, dock, etc.)*
9. Mailing Address Street or P.O. Box
City State Zip Code County
23. Address Where Injury or Exposure Occurred Name of business if incident
occurred on a business site
Street or P.O. Box County
10. Marital Status
Married Widowed Separated Single Divorced
City State Zip Code
11. Number of Dependent Children 12. Spouse's Name
24. Cause of Injury (fall, tool, machine, etc.)*
13. Doctor's Name Telephone # 25. List Witnesses (Name, Telephone #
14. Doctor's Mailing Address (Street or P.O.Box)
City State Zip Code
26. Return to work
date (m-d-y)
27. Did employee
die?
YES NO
28. Supervisor's
Name
29. Date Reported
(m-d-y)
30. Date of Hire (m-d-y)
31. Was employee hired or recruited in Texas?
YES NO
32. Length of Service in Current Position
Years
Months ______
33. Length of Service in Occupation
Years
Months ______
34. State Payroll Classification Code
35. Occupation of Injured Worker
36. Rate of Pay at this Job
$______ Hourly $
Weekly
$
Monthly
37. Full Work Week is:
Hours Days
38. Last Paycheck was:
$_____________
39. Is employee an Owner, Partner,
or Corporate Officer?
YES NO x
40. Name and Title of Person Completing Form
Claim s Coordinator
41. Name of Agency
42. Agency Mailing Address and Telephone Number
Street or P.O. Box Telephone
( )
43. Agency Location Code
______ ______ ______ / _______ ______ _______ / ______ _______ _______
City State Zip Code
Name of Location: ____________________________________________
44. Federal Tax Identification Number 45. Primary North American Industrial Classification System
Sector Code (NAICS) (2 digits)
46. Specific NAICS Code 47. Comptroller Agency Code
48. Workers' Comp
State Office of Risk Management
ensation Insurance Company 49. Policy Number
TXSTATEPOL001
50. Did you request accident prevention services in past 12 months?
YES NO If yes, did you receive them? YES NO
52. Number of Hours of Sick/Annual Leave Credted to Employee or Date of Injury
51. Signature and Tit le (READ INSTRUCTIONS ON INSTRUCTION SHEET BEFORE SIGNING)

DWC FORM-1S Instructions
PLEASE COMPLETE ALL APPLICABLE FIELDS. Most fields are self-explanatory; howev er, the following items may require
more attention:
Item 4: If no home phone, please give a phone n umber where the employee can be reach ed.
Item 7: Employees work phone numbe r.
Item 8: This information is no longer required.
Item 13: This information should includ e the doctor’s telephone nu mber.
Item 15: This should be the actual date of injury, or (for occupational diseases) the date the employee knew or should have
known the condition was work-related.
Item 17: This should be the first full day of lost-time from work. (Please note that the date of injury is not considered the first day
of lost time.) Mark NLT or N/A if there is no lost time.
Item 18: List the nature of the injury. Examples include: burn, cut, or sprain.
Item 19: List specific body part, which side of body is affected, e.g., chin, right leg, left upper arm, etc. If more than o ne body
part is affected, list each part.
Item 20: Describe in detail. Use additional sheet of paper if necessary.
Item 24: This should state the spe cific substance or exposure that directly inflicted the injury such as a tool, chemical (list the
name of the chemical), or machine.
Item 26: The date should be entered even if the employee has returned to work even for a portion of the day. If the employee
has returned to work making less than his or her pre-injury wage, a DWC FORM-6 must also be su bmitted.
Item 28: This is the employee’s immediate supervisor. Please include a work telepho ne number.
Item 29: This is the date the employee reported the injury to the employer as wo rk related.
Item 34: This 4-digit code corresp onds to the primary occupation in which the employee was engaged at the time of the injury or
exposure. This code is from the state payroll classification table and is available from the State Comptroller of Public Accounts.
Item 43: This 9-digit code represents the location of the agency unit that employed the injured worker at the time of their injury or
exposure. The first three digits will be 100 for state agencies or 200 for county entities. The second three digits are the agency
code. The third three digits are the location code as established by each agency. Conta ct the SORM’s Risk Assessment and
Loss Prevention section for information about or changes to your agency location cod e(s).
Item 44: This 9-digit code is assigned to each agency by the Internal Revenue Service for employment, tax, and repo rting
purposes.
Item 45: This 2-digit code is assigned to each agency accordi ng to its primary busine ss activity. For specific questions regarding
your NAICS code, call your local Texas Wo rkforce Commission (TWC).
Item 46: This is a 3- or 4-digit code for the specific subsector of the business activity of the agency.
Item 47: This is the state agency code number assigned by the State Comptroller of Public Accounts.
Item 51: This must be the signature and title of the claims coordinator. If signed by someone other than the claims coordinator,
he or she must list his or her title and state that it was sig ned for the claims coordinator. The date must also be included.
Item 52: Enter the number of sick/annual leave hours credited to the employee as of the date of injury.
Distribution: State Office of Risk Management
Fax a copy or mail the original to: P.O. Box 13777
State Office of Risk Management Austin, TX 78711-3777
Mail a copy to the claimant.
Retain a copy for your file.
DWC FORM-1S (Rev. 10/05) Page 2 DIVISION OF WORKERS’ COMPENSATION


