
Fillable Printable Health Care Proxy Form Instructions - New York
Fillable Printable Health Care Proxy Form Instructions - New York

Health Care Proxy Form Instructions - New York
Health
Care
Proxy Form Instructions
Item
(1)
Write the name, home address and telephone
number
of the
person you
are
selecting as
your
agent.
Item
(2)
If
you
want to appoint an alternate
agent, write the
name, home address and telephone
number
of the
person you
are selecting as
your
alternate agent.
Item
(3)
Your Health
Care
Proxy will
remain
valid
indefinitely unless
you
set an expiration date or
condition
for its expiration. This section
is
optional
and should be
filled in
only
if
you
want
your
Health
Care
Proxy
to expire.
Item
(4)
If
you
have
special
instructions
for
your
aEient, write
them here.
Also, if
you
wish
to limit
your
agent's
authority in any way,
you
may say so
here
or discuss
them with
your
health care agient.
If
you
do not
state any
limitations,
your
agent will be allowed to
make
all
health care decisions that
you
could have
made, including the decision to
consent to or
refuse
life-sustaining treatment.
If
you
want
to
give
your
agent
broad authority,
you
may
do so
right on the
form.
Simply write:
I
haue
discussed my wishes
uith my health care
agent
and
alternate and
they know my wishes
including those
about artificial nutrition
and hydration.
If
you
wish to
make more specific
instructions,
you
could say:
If I
become terminally
ill,
I
doldon't
want to
receiue
the following types of treatments....
If I am in a coma or haue
little conscious
understanding,
with no hope of
recot)eru, then
I
dol
don't want the
following types of treatments:....
If I
haue brain damage
or a brain disease
that
makes me unable to
recognize
people
or
speak and
there is no
hope that my condition
will improue,
I
doldon't want
the following types
of treatments:....
I haue
discussed
with mg agent
mg wishes
about and
I
want
mg agent
to
make
all decisions about these
measures.
30
Examples of medical treatments about which
you
may
wish
to
give
your
aEient special
instructions
are
listed
below.
This is not a complete list:
.
artificial
respiration
.
artificial nutrition and
hydration
(nourjshment
and water
provided
by
feeding
tube)
.
cardiopulmonary
resuscitation
(CPR)
.
antipsychotic medication
o
electric
shock therapy
o
antibiotics
.
surgical
procedures
.
dialysis
.
transplantation
.
blood transfusions
.
abortion
.
sterilization
Item
(5)
You
must date and sign
this Health Care
Proxy
form. If
you
are unable to
sign
yourself,
you
may
direct someone else to sign
in
your
presence.
Be
sure to
include
your
address.
Item
(6)
You may state wishes or
instructions about organ
and /or tissue
donation on this
form. New York
law does
provide
for
certain
individuals
in
order
of
priority
to consent to an
organ and/or tissue
donation
on
your
behalf:
your
health
care
agent,
your
decedent's agent,
your
spouse
,
if
you
are
not legally separated, or
your
domestic
partner,
a
son or daughter
18
years
of agie or older,
either of
your parents,
a brother or sister
18
years
ofage
or
older, a
guardian
appointed by a court
prior
to the
donor's
death.
Item
(7)
TVro witnesses
18
years
of age
or older must sign
this
Health Care
Proxy form.
The
person
who
is
appointed
your
agent or alternate
agient cannot
sign as a witness.
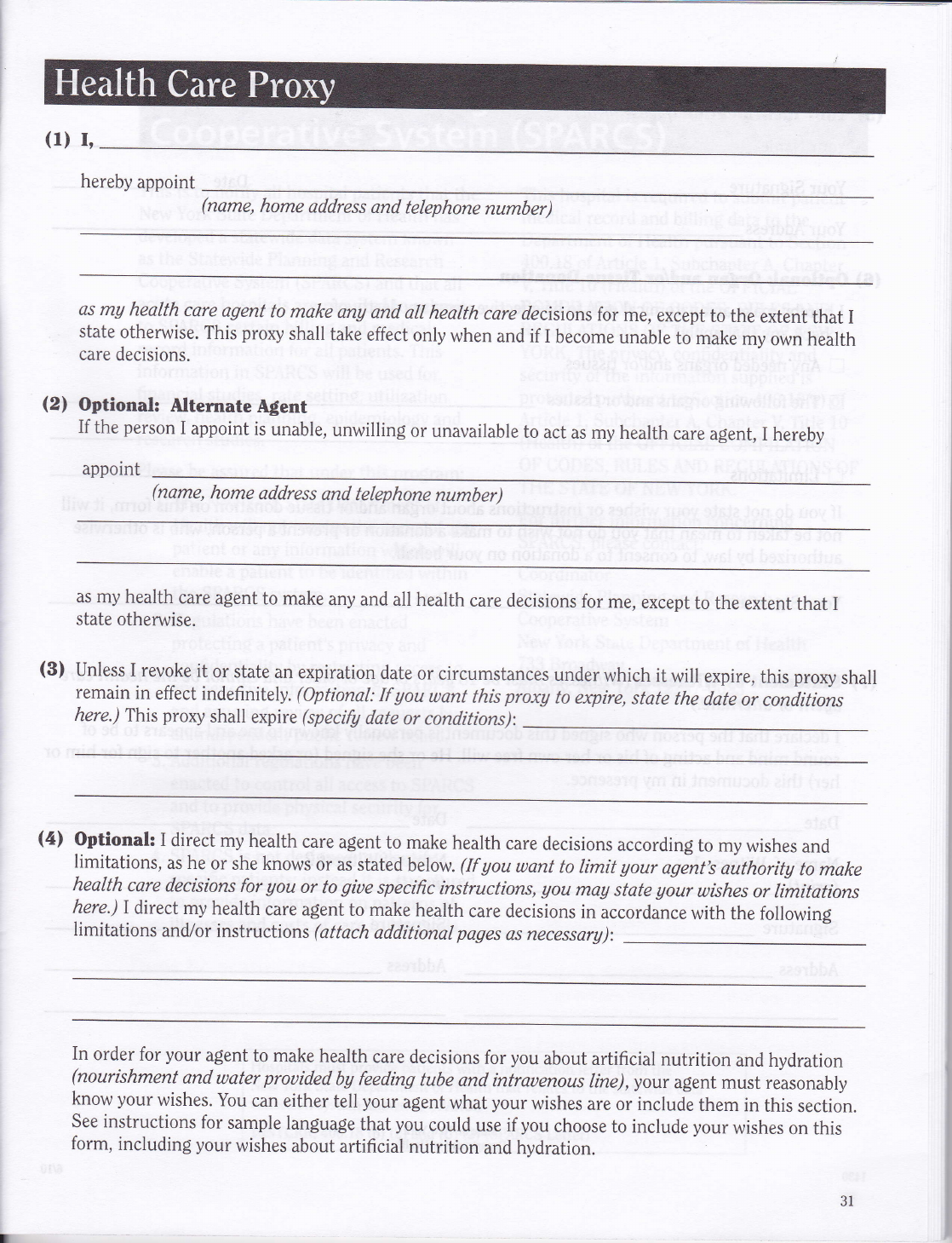
(1)
r,
hereby
appoint
(name,
home
address
and
telephone
number)
as
mU
health
care
agent
to
make
any
and
all
health
care
decisions
for
me,
except
to the
extent
that
I
state
otherwise.
This
pro)ry
shall
take
effect
only
when
and if I
become
unable
tomake
my
own
health
care
decisions.
(2)
Optional:
Nternate
Agent
If
the
person
I
appoint
is
unable,
unwilling
or
unavailable
to
act
as my
health
care
agent,
I hereby
appoint
(name,
home
address
and
telephone
number)
as my health
care
agient
to make
any
and all
health
care decisions
for
me,
except
to
the extent
that I
state
otherwise.
(3)
Unless
I
revoke
it
or state
an
expiration
date
or
circumstances
under
which
it
will
expire,
this
proxy
shall
remain
in
effect
indefinitely.
(Optional:
If
you
want
this
proxA
to
expire,
state
the
date
or conditions
here.)
This
proxy
shall
expire
(specify
date
or
conditions):
(4t
Optionak
I
direct
my
health
care
agent
to
make
health
care
decisions
according
to my
wishes
and
limitations,
as he
or
she knows
or
as stated
below.
(If
you
want
to limit
gour
agentb
authority
to
make
health
care
decisions
for
gou
or
to
giue
specific
instructions,
Uou
mag state
gour
wishes
or
limitations
here.)I
direct my
health
care
agent
to make
health
care
decisions
in
accordince
with
the following
limitations
and/or instructions
(attach
additionat
pages
as
necessarg):
In
order
for
your
agent
to
make
health
care
decisions
for
you
about
artificial
nutrition
and hydration
(nourishment
and
water
prouided
bg feeding
tube
and
intrauenous
line),
your
agent must
reasonably
know
your
wishes.
You
can
either
tell
your
agent
what
your
wishes
are or include
them in
this
section.
See instructions
for
sample
language
that
you
could
use if
you
choose
to include
your
wishes
on this
form,
including
your
wishes
about
artificial
nutrition
and hydration.
i
h,
31

(5)
Your Identlfication
(please
print)
Your Name
Your Signature
Date
Your Address
(6)
Optional:
Organ
and/or
Tissue
Donation
I hereby
make an anatomical
gift,
to be effective upon
my death, of:
(check
any
that apply)
tr
Any
needed organs and/or
tissues
I
The
following organs
and/or
tissues
E
Limitations
If
you
do
not state
your
wishes
or instructions
about
orEian and/or
tissue
donation
on this
form, it will
not
be
taken to
mean that
you
do
not wish to
make a
donation or
prevent
a
person,
who is otherwise
authorized
by
law,
to
consent
to a donation
on
your
behalf.
Your
Signature
(7)
Statement
by
Witnesses
(Witnesses
must
be 18
years
of age
or older
and cannot
be the health
care
agent or alternate.)
I declare
that the
person
who signed
this document
is
personally
known
to me and
appears to
be of
sound
mind and acting
of
his or
her own
free
will.
He
or she signed
(or
asked
another
to sign
for him or
her) this document
in my
presence.
Date
Date
Name of Witness
1
Name of Witness
2
(print)
(print)
Date
Signature
Address
Signature
Address
State of
NewYork
Department
of
Health
1430
32
6/10


