
Fillable Printable Incapacitation Pay Monthly Claim Form
Fillable Printable Incapacitation Pay Monthly Claim Form
Incapacitation Pay Monthly Claim Form
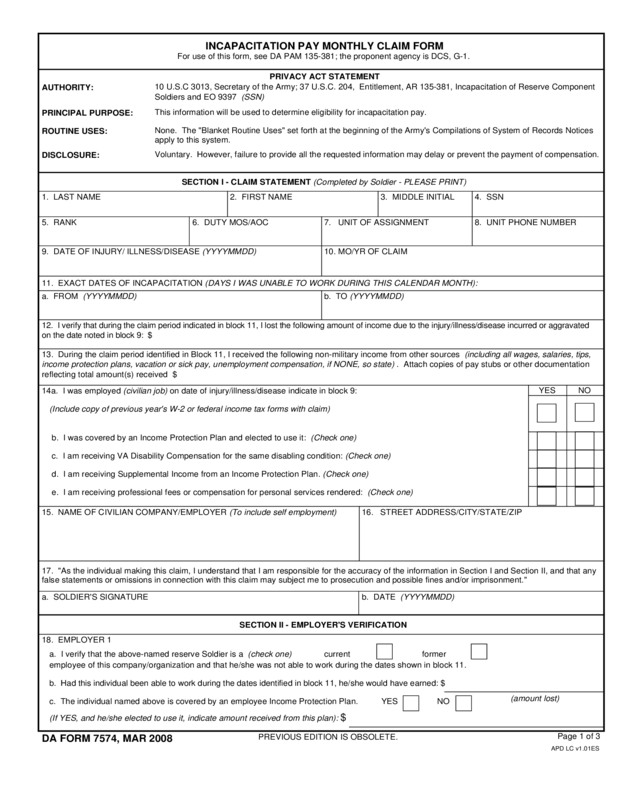
13. During the claim period identified in Block 11, I received the following non-military income from other sources (including all wages, salaries, tips,
income protection plans, vacation or sick pay, unemployment compensation, if NONE, so state) . Attach copies of pay stubs or other documentation
1. LAST NAME 2. FIRST NAME 3. MIDDLE INITIAL
5. RANK 6. DUTY MOS/AOC 7. UNIT OF ASSIGNMENT
4. SSN
8. UNIT PHONE NUMBER
9. DATE OF INJURY/ ILLNESS/DISEASE (YYYYMMDD)
10. MO/YR OF CLAIM
a. FROM (YYYYMMDD) b. TO (YYYYMMDD)
12. I verify that during the claim period indicated in block 11, I lost the following amount of income due to the injury/illness/disease incurred or aggravated
on the date noted in block 9: $
15. NAME OF CIVILIAN COMPANY/EMPLOYER (To include self employment)
16. STREET ADDRESS/CITY/STATE/ZIP
a. SOLDIER'S SIGNATURE
b. DATE (YYYYMMDD)
INCAPACITATION PAY MONTHLY CLAIM FORM
For use of this form, see DA PAM 135-381; the proponent agency is DCS, G-1.
APD LC v1.01ES
Page 1 of 3
DA FORM 7574, MAR 2008
PREVIOUS EDITION IS OBSOLETE.
PRIVACY ACT STATEMENT
AUTHORITY:
PRINCIPAL PURPOSE:
ROUTINE USES:
DISCLOSURE:
10 U.S.C 3013, Secretary of the Army; 37 U.S.C. 204, Entitlement, AR 135-381, Incapacitation of Reserve Component
Soldiers and EO 9397 (SSN)
This information will be used to determine eligibility for incapacitation pay.
Voluntary. However, failure to provide all the requested information may delay or prevent the payment of compensation.
SECTION I - CLAIM STATEMENT (Completed by Soldier - PLEASE PRINT)
11. EXACT DATES OF INCAPACITATION (DAYS I WAS UNABLE TO WORK DURING THIS CALENDAR MONTH):
SECTION II - EMPLOYER'S VERIFICATION
b. I was covered by an Income Protection Plan and elected to use it: (Check one)
c. I am receiving VA Disability Compensation for the same disabling condition: (Check one)
d. I am receiving Supplemental Income from an Income Protection Plan. (Check one)
e. I am receiving professional fees or compensation for personal services rendered: (Check one)
18. EMPLOYER 1
(If YES, and he/she elected to use it, indicate amount received from this plan):
$
a. I verify that the above-named reserve Soldier is a (check one)
c. The individual named above is covered by an employee Income Protection Plan.
current former
employee of this company/organization and that he/she was not able to work during the dates shown in block 11.
YES NO
b. Had this individual been able to work during the dates identified in block 11, he/she would have earned: $
(amount lost)
14a. I was employed (civilian job) on date of injury/illness/disease indicate in block 9:
YES NO
None. The "Blanket Routine Uses" set forth at the beginning of the Army's Compilations of System of Records Notices
apply to this system.
reflecting total amount(s) received $
(Include copy of previous year's W-2 or federal income tax forms with claim)
17. "As the individual making this claim, I understand that I am responsible for the accuracy of the information in Section I and Section II, and that any
false statements or omissions in connection with this claim may subject me to prosecution and possible fines and/or imprisonment."
LAST NAME
e. EMPLOYER'S REPRESENTATIVE (Name, title,
business address)
33. REMARKS
FIRST NAME MIDDLE INITIAL SSN
i. SIGNATURE/DATE
f. PHONE NUMBER h. EMAIL ADDRESS
g. FAX NUMBER
32. NAME/RANK/TITLE/SIGNATURE/DATE (Approving Authority)
29. POINT OF CONTACT (Name, title, email address, Fax number)
28. JFHQ/USARC/RRC/MSC
e. EMPLOYER'S REPRESENTATIVE (Name, title,
business address)
i. SIGNATURE
f. PHONE NUMBER h. EMAIL ADDRESS
g. FAX NUMBER
30. PHONE NUMBER
20. UNIT OF ASSIGNMENT
21. UNIT ADDRESS (CITY, STATE, ZIP CODE)
22. UIC 23. SOLDIER'S DUTY MOS/AOC
24. SUPPORTING MILITARY MEDICAL TREATMENT FACILITY OR COMMAND AND ADDRESS
26. COMMANDER'S NAME/RANK/SIGNATURE/DATE
31.
SECTION II - EMPLOYER'S VERIFICATION (Continued)
Page 2 of 3
DA FORM 7574, MAR 2008
19. EMPLOYER 2 (If applicable)
a. I verify that the above-named reserve Soldier is a (check one)
current former
employee of this company/organization and that he/she was not able to work during the dates listed in block 11 of this form.
b. Had this individual been able to work during the dates above, he/she would have earned: $
(amount lost)
c. Is the individual named above covered by an employee Income Protection Plan? YES NO
(If YES, and elected to use it, indicate amount he/she received from this plan): $
d. I understand that this information is being used by the claimant as the basis of a claim against the United States government. I further
understand that knowingly and willfully assisting a claimant making a false claim or statement in connection with a claim is a criminal
offense under Federal and State laws which may subject the parties to a substantial fine and/or lengthy improvement.
SECTION III - COMMANDER'S VERIFICATION
SECTION IV - REVIEW / APPROVAL
APPROVED
DISAPPROVED
27. I have reviewed the approved line of duty investigation (IAW AR 600-8-4) which is attached (Commander's Initials):
25. DETERMINED UNFIT FOR MILITARY DUTY: I,
RECOMMEND APPROVAL
RECOMMEND DISAPPROVAL (See Attached)
paid for duty after being determined unfit to perform military duty.
(Soldier's Name) , have not performed or been
(Soldier's Signature).
d. I understand that this information is being used by the claimant as the basis of a claim against the United States government. I further understand that
knowingly and willfully assisting a claimant making a false claim or false statement in connection with a claim is a criminal offense under Federal and
State laws which may subject the parties to a substantial fine and/or lengthy imprisonment.
APD LC v1.01ES
SECTION IV - REVIEW/APPROVAL
DA FORM 7574, MAR 2008
Page 3 of 3
INCAPACITATION PAY MONTHLY CLAIM FORM
INSTRUCTION SHEET
SECTION I - CLAIM STATEMENT
1. Self-explanatory.
2. Self-explanatory.
3. Self-explanatory.
4. Self-explanatory.
5. Rank -PVT, SPC, SGT, 1LT, CW2, CPT, COL
6. Duty MOS/AOC - 91B, 13B, 42D/66H, 70B.
7. Self-explanatory.
8. Self-explanatory.
9. Date of Injury/Illness/Disease (YYYYMMDD).
10. Month/Year of Claim (MM/YY or Claim) - 11/98, 12/98 or 03/00.
14.a. Indicate whether you were employed (check Yes) or unemployed
(check No).
14.b. Self-explanatory.
15. Self-explanatory.
16. Self-explanatory.
SECTION II - EMPLOYER'S VERIFICATION
18. EMPLOYER 1
a. Self-explanatory.
c. Self-explanatory.
d. Self-explanatory.
e. f., g., h., i. Self-explanatory.
19. EMPLOYER 2
a., b., c., d., e., f., g., h., i. Same as 18.a THRU e above.
SECTION III - COMMANDER'S VERIFICATION
20. Self-explanatory.
21. Self-explanatory.
22. Unit Identification code (UIC).
23. Same as block 6.
24. Self-explanatory.
25. Self-explanatory.
26. Self-explanatory.
31. Self-explanatory.
32. Self-explanatory.
33. Self-explanatory.
28. Higher headquarters or approving authority
(JFHQ/USARC/RRC/MSC).
29. Point of contact within STARC/USARC/RRC/MSC.
30. Self-explanatory.
27. Commander's Initials.
11. Exact Dates of Incapacitation - Do not cross calendar months
when completing this form. This first date of incapacitation will be the
date the government physician determines the Soldier unfit for military
duty or demonstrates a loss of nonmilitary income. Subsequent the
Incapacitation Pay Monthly Claim Form will reflect the entire month,
i.e., 1 Sep 99 to 30 Sep 99 or 1 Oct 99 to 31 Oct 99 or the end of the
incapacitation claim.
12. Amount of income, from civilian job, which you would have earned
if you had not been injured. This must be during the claim period
indicated on the Incapacitation Pay Monthly Claim Form. NOTE: Full
months of incapacitation pay and allowances are based on a
calculation of 30 days per month, regardless of the actual days per
month.
13. Amount of reportable income from other sources that you received
during the incapacitation period reflected in Block II.
14. c. You must indicate whether or not you are receiving VA
Disability Compensation for the same condition. If you are, the amount
of the compensation will be deducted from your incapacitation
entitlements.
Disability Compensation for the same condition. If you are, the amountof the compensation will be deducted from your incapacitation
14. d. Indicate whether receiving Supplemental Income from an Income
Protection Plan. If you are, that amount will be deducted.
14. e. Indicate whether receiving professional fees or compensation for
other personal services rendered. If you are, that amount will be
deducted.
17. Your signature indicates all previous statements are true and
accurate and that you may be subject to prosecution for making
false claims.
b. Amount this employee would have earned if he/she were able to
work.
APD LC v1.01ES


