
Fillable Printable Initial Medical Review - Annual Medical Certificate
Fillable Printable Initial Medical Review - Annual Medical Certificate
Initial Medical Review - Annual Medical Certificate
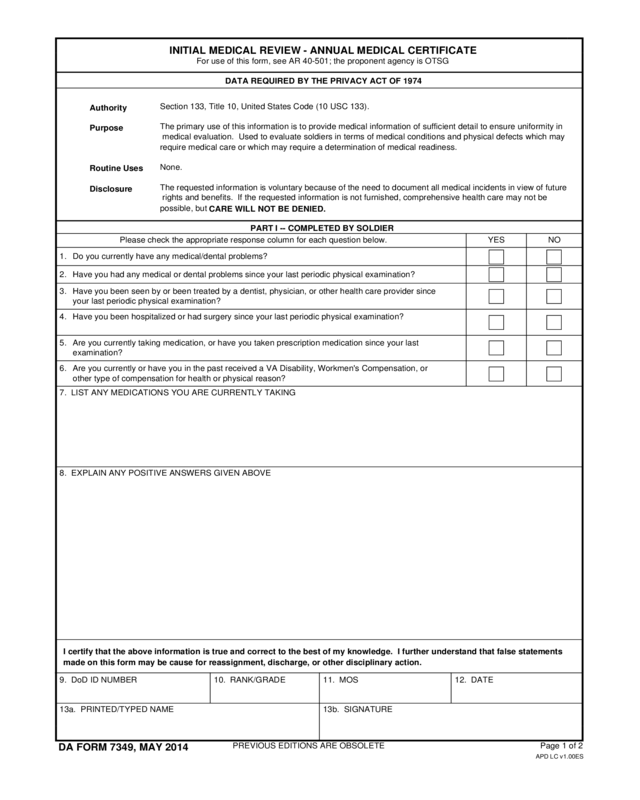
INITIAL MEDICAL REVIEW - ANNUAL MEDICAL CERTIFICATE
DATA REQUIRED BY THE PRIVACY ACT OF 1974
PART I -- COMPLETED BY SOLDIER
Authority
Purpose
Routine Uses
Disclosure
Section 133, Title 10, United States Code (10 USC 133).
Please check the appropriate response column for each question below. YES NO
Do you currently have any medical/dental problems?1.
Have you had any medical or dental problems since your last periodic physical examination?2.
3.
Have you been hospitalized or had surgery since your last periodic physical examination?4.
5.
6.
DA FORM 7349, MAY 2014
7. LIST ANY MEDICATIONS YOU ARE CURRENTLY TAKING
8. EXPLAIN ANY POSITIVE ANSWERS GIVEN ABOVE
9. DoD ID NUMBER 10. RANK/GRADE 11. MOS 12. DATE
13a. PRINTED/TYPED NAME 13b. SIGNATURE
PREVIOUS EDITIONS ARE OBSOLETE
APD LC v1.00ES
For use of this form, see AR 40-501; the proponent agency is OTSG
possible, but
CARE WILL NOT BE DENIED.
The primary use of this information is to provide medical information of sufficient detail to ensure uniformity in
medical evaluation. Used to evaluate soldiers in terms of medical conditions and physical defects which may
require medical care or which may require a determination of medical readiness.
None.
The requested information is voluntary because of the need to document all medical incidents in view of future
rights and benefits. If the requested information is not furnished, comprehensive health care may not be
Have you been seen by or been treated by a dentist, physician, or other health care provider since
your last periodic physical examination?
Are you currently taking medication, or have you taken prescription medication since your last
examination?
Are you currently or have you in the past received a VA Disability, Workmen's Compensation, or
other type of compensation for health or physical reason?
I certify that the above information is true and correct to the best of my knowledge. I further understand that false statements
made on this form may be cause for reassignment, discharge, or other disciplinary action.
Page 1 of 2
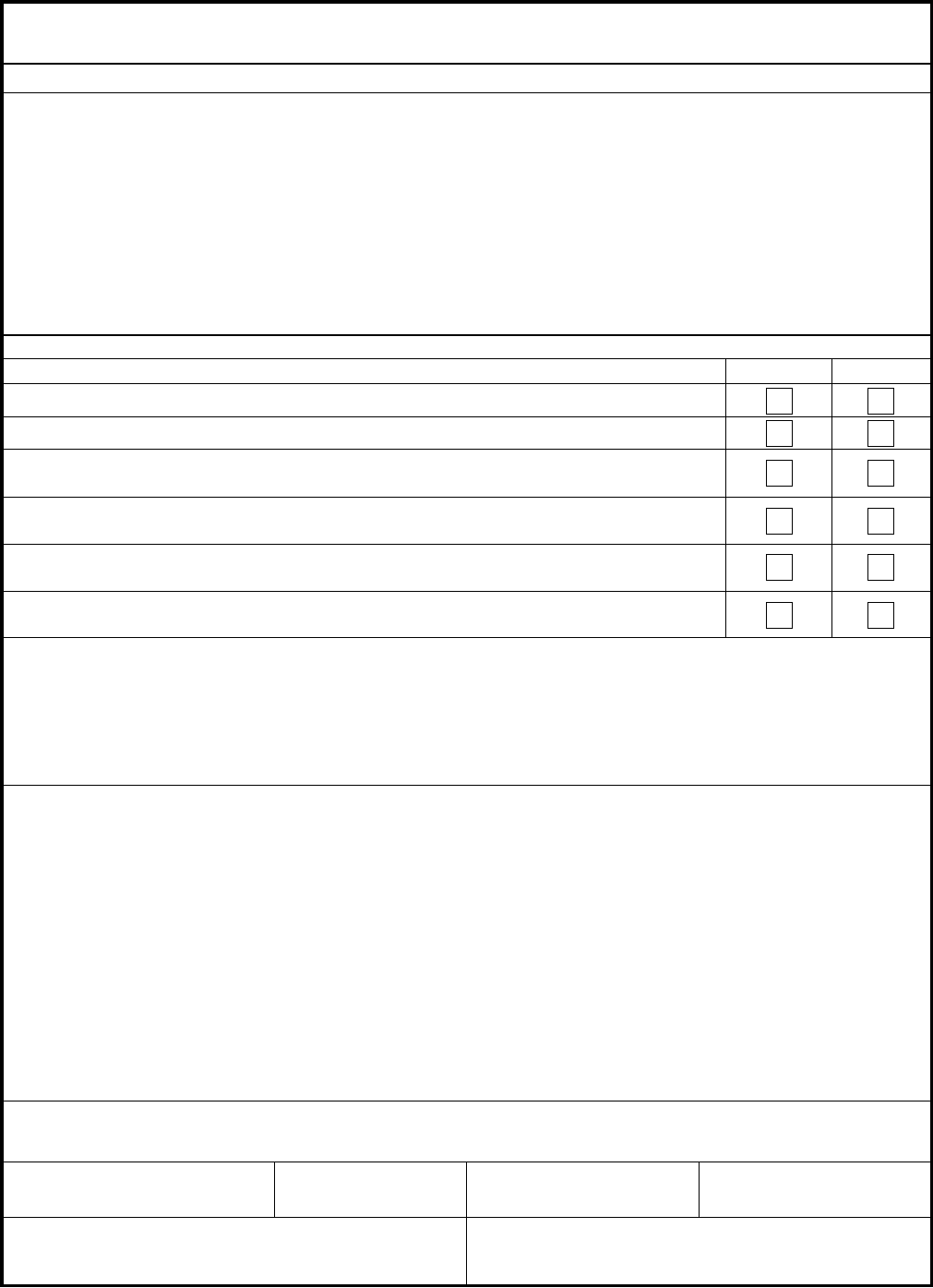
PART II -- COMPLETED BY INITIAL REVIEWER
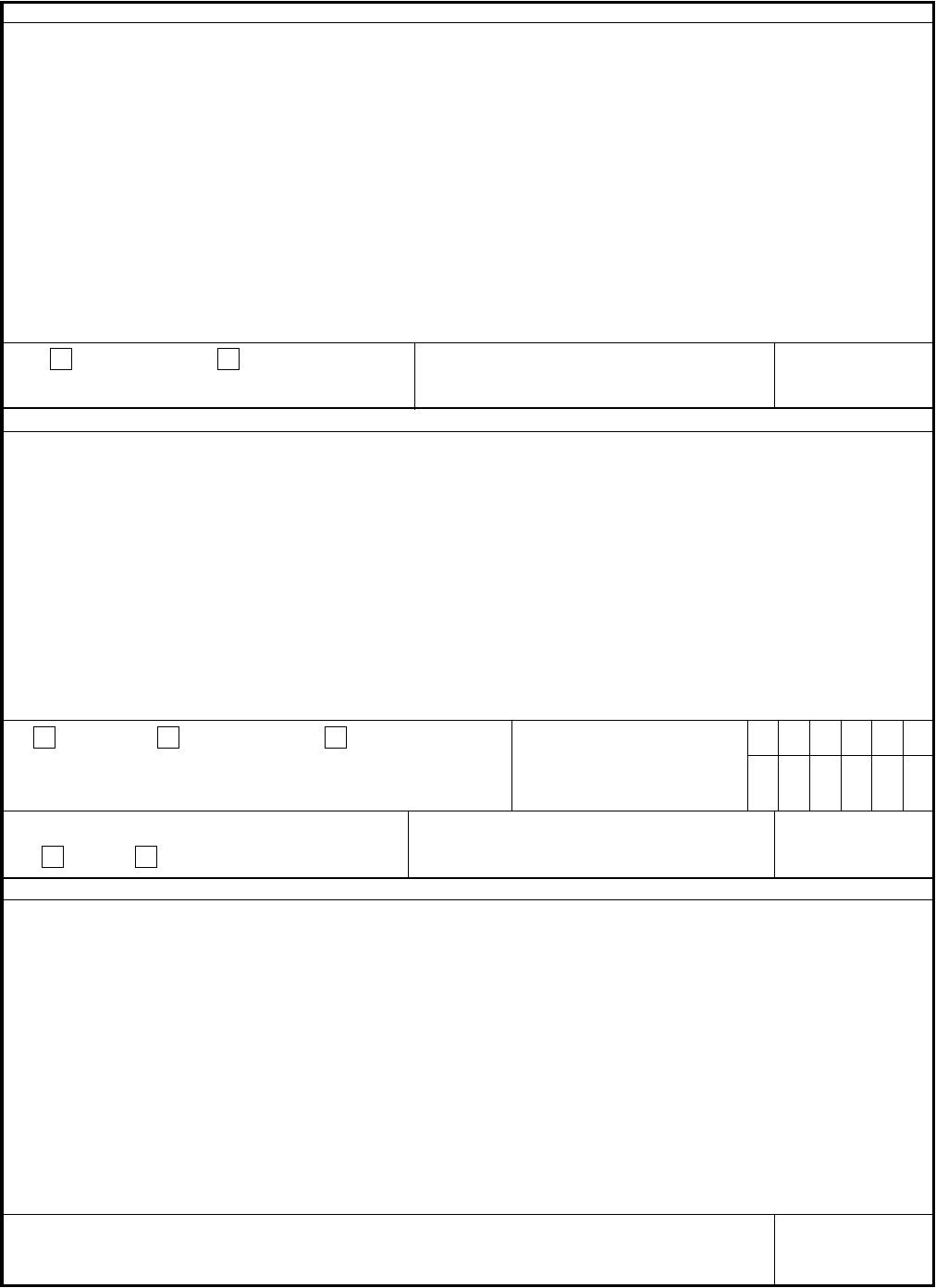
DA FORM 7349, MAY 2014 (BACK)
15. MEDICALLY REQUIRES
FURTHER
EVALUATION
PART III -- COMPLETED BY PHYSICIAN
19. MEDICALLY
NOT MEDICALLY
READY (USAR
refer to para 9-10 &
9-11 AR 40-501)
NOT MEDICALLY
READY (Army National
Guard refer to MDRB)
20. Complete "PULHES" using the
Physical Profile Functional
Capacity Guide in Table 7-1,
AR 40-501.
P
U
L H E
S
21. DA FORM 3349 IS ATTACHED
YES
NO
PART IV -- COMPLETED BY APPROVING AUTHORITY
14. INITIAL REVIEWER'S NOTES
16. SIGNATURE 17. DATE
18. PHYSICIAN'S REVIEW NOTES
22. SIGNATURE 23. DATE
24. MISCELLANEOUS RECOMMENDATIONS
25. SIGNATURE 26. DATE
APD LC v1.00ES
READY
READY
Page 2 of 2


