
Fillable Printable Inpatient Treatment Record Cover Sheet
Fillable Printable Inpatient Treatment Record Cover Sheet
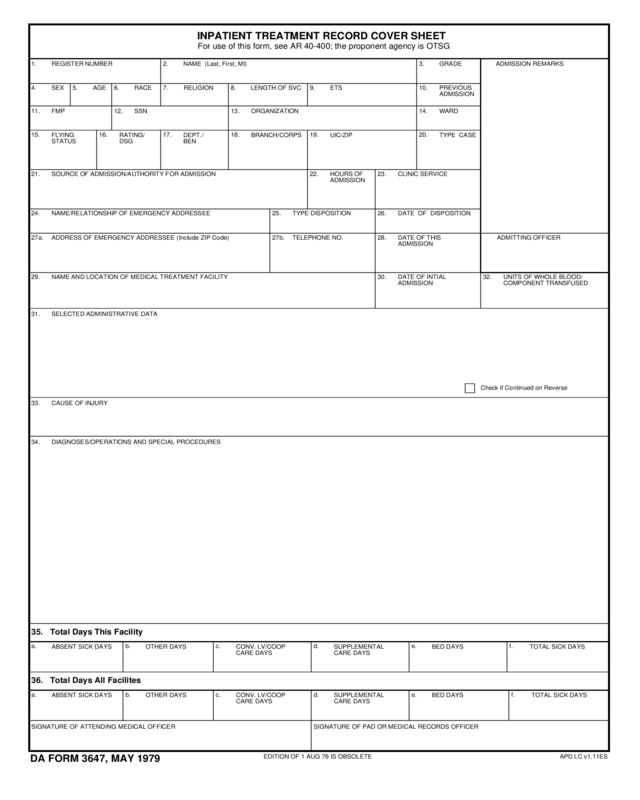
Inpatient Treatment Record Cover Sheet
34.
SIGNATURE OF ATTENDING MEDICAL OFFICER
30.
SIGNATURE OF PAD OR MEDICAL RECORDS OFFICER
10.
b.
32.
17.
d.a.
29.
2. 3.1.
22.
18.
f.
f.e.
e.
c.
c. d.b.a.
31.
23.
27a.
24.
21.
27b.
25.
28.
26.
20.19.16.15.
13.
8.
14.11. 12.
7.4. 6. 9.5.
33.
For use of this form, see AR 40-400; the proponent agency is OTSG
ADMITTING OFFICER
36. Total Days All Facilites
35. Total Days This Facility
ABSENT SICK DAYS
ADMISSION REMARKS
OTHER DAYS
ABSENT SICK DAYS
NAME/RELATIONSHIP OF EMERGENCY ADDRESSEE
HOURS OF
ADMISSION
SELECTED ADMINISTRATIVE DATA
NAME AND LOCATION OF MEDICAL TREATMENT FACILITY
ADDRESS OF EMERGENCY ADDRESSEE (Include ZIP Code)
SOURCE OF ADMISSION/AUTHORITY FOR ADMISSION
TELEPHONE NO.
TYPE DISPOSITION
BRANCH/CORPS
ORGANIZATION
LENGTH OF SVC
WARDFMP
RACE
BED DAYS
OTHER DAYS
DATE OF DISPOSITION
CLINIC SERVICE
TYPE CASEUIC/ZIP
SSN
GRADEREGISTER NUMBER
SEX ETS RELIGIONAGE
Check if Continued on Reverse
TOTAL SICK DAYS
TOTAL SICK DAYSBED DAYS
NAME (Last, First, MI)
DIAGNOSES/OPERATIONS AND SPECIAL PROCEDURES
CAUSE OF INJURY
DA FORM 3647, MAY 1979
EDITION OF 1 AUG 76 IS OBSOLETE APD LC v1.11ES
INPATIENT TREATMENT RECORD COVER SHEET
DATE OF INTIAL
ADMISSION
UNITS OF WHOLE BLOOD/
COMPONENT TRANSFUSED
DATE OF THIS
ADMISSION
PREVIOUS
ADMISSION
RATING/
DSG
DEPT./
BEN
FLYING
STATUS
CONV. LV/COOP
CARE DAYS
SUPPLEMENTAL
CARE DAYS
SUPPLEMENTAL
CARE DAYS
CONV. LV/COOP
CARE DAYS
APD LC v1.11ES


