
Fillable Printable Labor Certified Transcript of Payroll - Illinois
Fillable Printable Labor Certified Transcript of Payroll - Illinois
Labor Certified Transcript of Payroll - Illinois
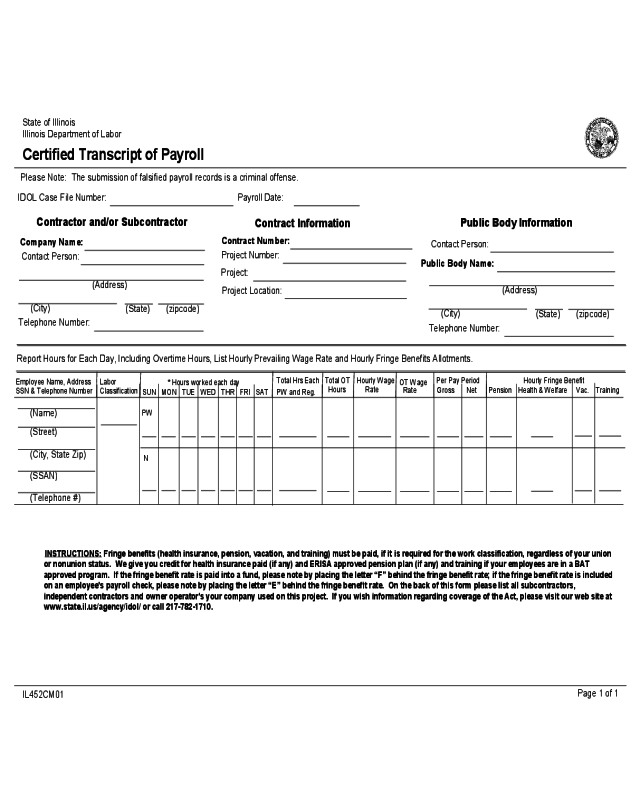
State of Illinois
Illinois Department of Labor
Certified Transcript of Payroll
IL452CM01
Page 1 of 1
Please Note: The submission of falsified payroll records is a criminal offense.
IDOL Case File Number:
Payroll Date:
Company Name:
Contact Person:
(Address)
(City)
(State) (zipcode)
Telephone Number:
Contractor and/or Subcontractor
Contract Number:
Project Number:
Project:
Contract Information
Project Location:
Public Body Name:
Contact Person:
(Address)
(City)
(State) (zipcode)
Telephone Number:
Public Body Information
Report Hours for Each Day, Including Overtime Hours, List Hourly Prevailing Wage Rate and Hourly Fringe Benefits Allotments.
Employee Name, Address
SSN & Telephone Number
Labor
Classification
* Hours worked each day
SUN MON TUE WED THR FRI SAT
Total Hrs Each
PW and Reg.
Total OT Hourly Wage
OT Wage
Hours Rate
Rate
Per Pay Period
Gross Net
Hourly Fringe Benefit
Pension
Health & Welfare Vac. Training
(SSAN)
(Street)
(City, State Zip)
(Telephone #)
(Name)
PW
N
INSTRUCTIONS
:
Fringe benefits (health insurance, pension, vacation, and training) must be paid, if it is required for the work classification, regardless of your union
or nonunion status. We give you credit for health insurance paid (if any) and ERISA approved pension plan (if any) and training if your employees are in a BAT
approved program. If the fringe benefit rate is paid into a fund, please note by placing the letter “F” behind the fringe benefit rate; if the fringe benefit rate is included
on an employee's payroll check, please note by placing the letter “E” behind the fringe benefit rate. On the back of this form please list all subcontractors,
independent contractors and owner operator's your company used on this project. If you wish information regarding coverage of the Act, please visit our web site at
www.state.il.us/agency/idol/ or call 217-782-1710.


