
Fillable Printable Medical Record Consultation Sheet
Fillable Printable Medical Record Consultation Sheet
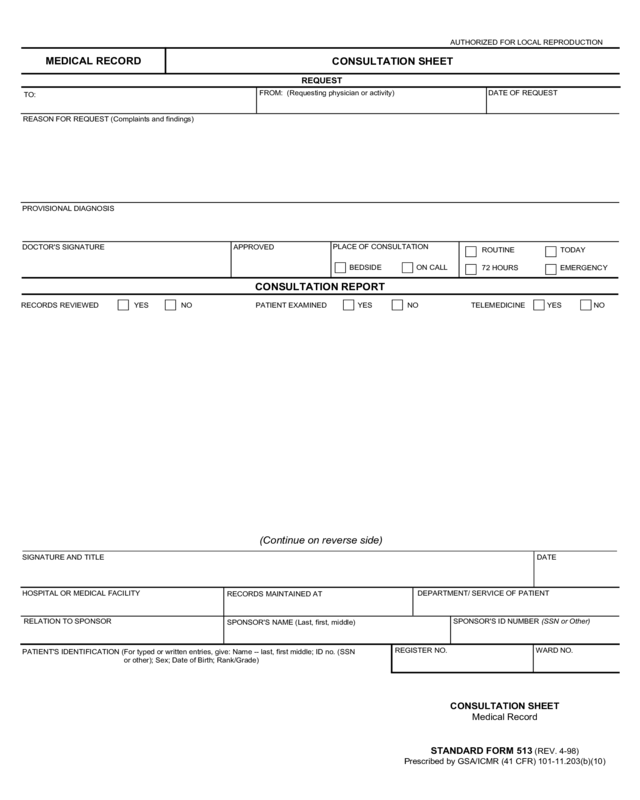
Medical Record Consultation Sheet
AUTHORIZED FOR LOCAL REPRODUCTION
MEDICAL RECORD
CONSULTATION SHEET
REQUEST
TO:
FROM: (Requesting physician or activity) DATE OF REQUEST
REASON FOR REQUEST (Complaints and findings)
PROVISIONAL DIAGNOSIS
DOCTOR'S SIGNATURE
APPROVED
PLACE OF CONSULTATION
BEDSIDE ON CALL
ROUTINE
72 HOURS
TODAY
EMERGENCY
CONSULTATION REPORT
RECORDS REVIEWED YES NO PATIENT EXAMINED YES NO TELEMEDICINE NOYES
(Continue on reverse side)
SIGNATURE AND TITLE DATE
HOSPITAL OR MEDICAL FACILITY
RECORDS MAINTAINED AT
DEPARTMENT/ SERVICE OF PATIENT
RELATION TO SPONSOR
SPONSOR'S NAME (Last, first, middle)
SPONSOR'S ID NUMBER (SSN or Other)
PATIENT'S IDENTIFICATION (For typed or written entries, give: Name -- last, first middle; ID no. (SSN
or other); Sex; Date of Birth; Rank/Grade)
CONSULTATION SHEET
Medical Record
STANDARD FORM 513 (REV. 4-98)
Prescribed by GSA/ICMR (41 CFR) 101-11.203(b)(10)
REGISTER NO. WARD NO.


