
Fillable Printable Notice Of Unemployment Insurance Award (De 429Z)
Fillable Printable Notice Of Unemployment Insurance Award (De 429Z)
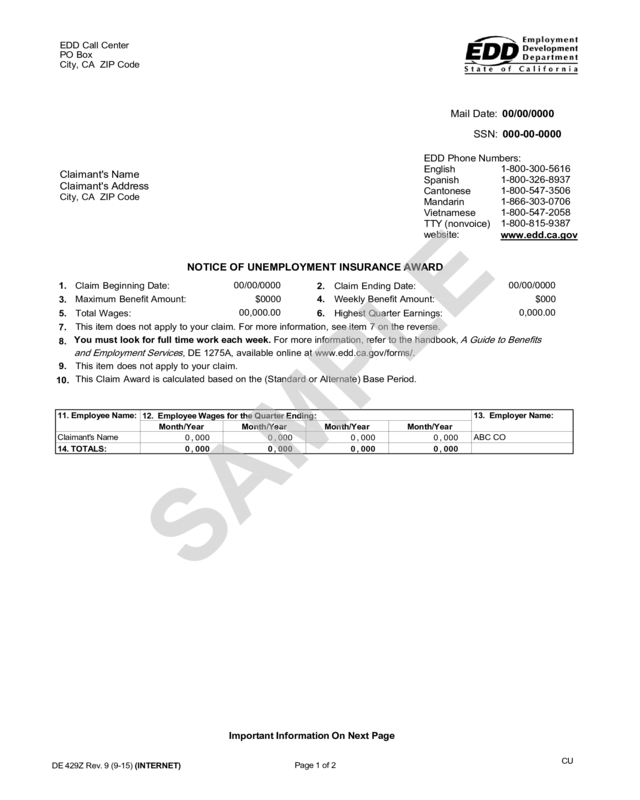
Notice Of Unemployment Insurance Award (De 429Z)

EDD Call Center
PO Box
City, CA ZIP Code
Mail Date: 00/00/0000
SSN: 000-00-0000
EDD Phone Numbers:
English
Spanish
Cantonese
Mandarin
Vietnamese
TTY (nonvoice)
website:
1-800-300-5616
1-800-326-8937
1-800-547-3506
1-866-303-0706
1-800-547-2058
1-800-815-9387
www.edd.ca.gov
Claimant's Name
Claimant's Address
City, CA ZIP Code
NOTICE OF UNEMPLOYMENT INSURANCE AWARD
Claim Beginning Date:
Maximum Benefit Amount:
Total Wages:
00/00/0000
$0000
00,000.00
2. Claim Ending Date:
00/00/0000
$000
0,000.00
1.
3.
5.
7.
8.
4.
Weekly Benefit Amount:
6. Highest Quarter Earnings:
This item does not apply to your claim. For more information, see item 7 on the reverse.
You must look for full time work each week. For more information, refer to the handbook,
A Guide to Benefits
and Employment
Services
, DE 1275A, available online at www.edd.ca.gov/forms/.
This item does not apply to your claim.
This Claim Award is calculated based on the (Standard or Alternate) Base Period.
9.
10.
Important Information On Next Page
DE 429Z Rev. 9 (9-15) (INTERNET)
Page 1 of 2
CU
11. Employee Name:
12. Employee Wages for the Quarter Ending:
13. Employer Name:
Month/Year Month/Year Month/Year Month/Year
Claimant's Name
0,000 0,000 0,000 0,000
ABC CO
14. TOTALS:
0,000 0,000 0,000 0,000
SAMPLE
DE 429Z Rev. 9 (9-15) Important Information On Next Page CU
THE FOLLOWING IS ADDITIONAL INFORMATIO N REGARDING THE ITEMS ON THE REVERSE OF THIS PAGE
1. Claim Beginni ng Date: The date your claim begins.
2. Claim Ending Date:
Thedateyourclaimends.
3. Maximum Benefit Amount:
The tot al amount of money y ou can receive from this claim .
4. Weekly Benefit Amount: The maximum amount you can be paid each week, if you m eet the weekly eligibility requirem ents.
5. To
tal Wages: The total amount of earnings reported by the empl oyer(s) during the quarters listed on the reverse page in i tem 12.
These ear nings were used to compute your maximum benefi t amount.
6. Highest Q
uarter Earnings: The calendar quarter list ed on t he reverse page in item 12 wit h the highest amount of ear nings. These
earnings deter mine your weekly benef it am ount.
7. The award listed on the reverse page in item 7 i s your award without the wages earned from a public or nonprofit school. If you
worked for a public or nonprofit school during any of the quarters listed on the reverse page in item 12, you may not be able to use
those wages in your claim during a school rec ess period.
8. You must foll ow the instructions on the reverse page in item 8 to be eligible for benefits. By law you must make al l r easonable efforts
to find work when claiming benef its.
9. The Unempl oyment Insurance Code (Section 1277) requires t hat you work between the beginning and the ending dates of a prior
claim to have a valid claim t he next year. If this applies to your claim you will receive additional instructions.
10. The type of base period used to establis h your claim; it will be ei ther t he Standard Base Period or the Alternate Base Period. If you
do not have sufficient wages in the Standard Base Period to establish a valid claim, you may be eligible to use the Alternate Base
Period. For more information, review the handbook, A GUIDE TO BENEFITS AND EMPLOYMENT SERVICES, DE 1275A, available
at www.edd.ca.gov/forms/
.
11. Employee
's Name: The name used by your employer(s) to report your earnings to the Employment Development Department (EDD)
during each calendar quarter list ed on t he reverse page in item 11.
12. Employee
'sWagesforthe Calendar Quarter Endi ng: These are the potentially usable wages f or unemployment insurance purposes
that your employer(s) reported you earned during each calendar quar ter listed. These earnings deter mi ne the amount of your
Unemployment Insurance (UI) award.
13. Employer Name: The name(s) of the empl oyer(s) you worked for during the cal endar quarters listed on the reverse page on item 13.
14. Totals :
The total amount of earnings reported by all employer(s) in each cal endar quarter listed on the reverse page in item 12.
YOUR CLAIM IS INVALID IF:
a. Your earnings were not enough to meet the minimum requirements.
b. You had a prior UI claim and did not meet the requirements for worki ng and earning wages necessary to have alatervalidclaim.
IMPORTANT:
Check this notice carefully to make sure that all empl oyers you worked for i n the calendar quarters shown, (on the reverse page in
item 12) are listed and t hat t he wages you earned are shown. If an employer is listed and you di d not work for them, or if an empl oyer is
not listed, or your wages are incorrect, contact an EDD office immediately t o protest t he accuracy of the computation. You may be
subject to disqualifications, overpayments, and/or cri mi nal penal ties for failure to notify the EDD immediately of any inaccurate
empl oyment and wage information displayed in item12.
If you worked for a federal agency your wages must be requested from that feder al agency. You will receive a Notice of Amended
Unemployment Insurance Awa
rd with these wages added.
If this notice or amended notice i s incorrect and you want to protest the accuracy of the computation or rec omput at ion, you must cont act
the EDD within 30 days after the m ail date of the notice or amended notice. Otherwise, a wage investi gation or recomputati on of wages
may be denied. The 30-day period may be extended for good cause. If you need to cont act the EDD, you will need to provide your f ull
name, address, and Social Securit y number and, if necessary, any wage and employment information you woul d like to add to your
claim, or to rem ove any employers for whom you did not work and earn wages.
YOU ARE RESPONSIBLE FOR KNOWING THE CONTENT OF THE UNEMPLOYMENT INSURANCE BENEFITS: WHAT YOU NEED
TO KNOW, DE 1275B, AND THE CONTENT OF THE HANDBOOK, A GUIDE TO BENEFITS AND EMPLOYMENT SERVICES,
DE 1275A. BOTH PUBLICATIONS EXPLAIN YOUR UNEMPLOYMENT RIGHTS AND RESPONSIBILITIES AND ARE AVAILABLE AT
WWW.EDD.CA.GOV/FORMS/
.
TO RECEIVE Ul BENEFITS, YOU MUST CERTIFY FOR BENEFITS USING ONE OF THE FOLLOWING M ETHODS: UI ONLINE
SM
,
EDD TELE-CERT
SM
, OR SUBMIT A PAPER CONTINUED CLAIM FORM, DE 4581. FOR MORE INFORMATION ON CERTIFYING
FOR BENEFITS, REFER TO THE DE 1275A HANDBOOK WHICH IS AVAILABLE ONLINE AT WWW.EDD.CA.GOV/FORMS/.
DE 429Z Rev.9 (9-15) (INTERNET)
Mail Date:
dte001
SSN:
str002
EDD Phone Numbers:
English 1-800-300-5616
Spanish 1-800-326-8937
Cantonese 1-800-547-3506
Mandarin 1-866-303-0706
Vietnamese 1-800-547-2058
TTY (nonvoice) 1-800-815-9387
website:
www.edd.ca.gov
11. Employee Name: 12. Employee Wages for the Quarter Ending: 13. Employer Nam e :
str037
str038 str039 str040
arr_str045
arr_str046 arr_str047 arr_str048 arr_str049
arr_str050
14. TOTALS:
str041
str042 str043 str044
1.
Claim Beginni ng Date: dte010
2.
Claim Ending Date: dte030
3.
Maximum Benefit Amount: str031
4.
Weekly Benefit Amount: str032
5.
Total Wages: str035
6.
Highest Quarter Earnings: str036
7.
str133
8.
rtf029a
9.
rtf057a
10.
This Claim Award is calculated based on the str158
Base Period.
str013
str014
str015 str016 str 017
str004 str005 str003
str006
str007 str008 str009
NOTICE OF str160UNEMPLOYMENT INSURANCE AWARD
SAMPLE
HOW TO CANCEL A UI CLAIM
You have an option of cancelling a regular California UI claim after you have been mailed your Unemployment Insurance Award
notice. If you want to cancel your claim, you need to contact the EDD right away. Do not certify for UI benefits using UI Online
SM
,
EDD Tele-Cert
SM
, or by submitting a paper Continued Claim Form, DE 4581. The law only allows you to cancel a UI claim if no benefits
have been paid, no notice of disqualification has been mailed to you, no overpayment has been established on the claim, and the
benefit year of your claim has not ended. If the claim is cancelled, it cannot be reopened. You must file a claim with a later date.
Page 2 of 2


