
Fillable Printable Notification Of Name Change Form
Fillable Printable Notification Of Name Change Form
Notification Of Name Change Form
STATE OF CALIFORNIA
DEPARTMENT OF CONSUMER AFFAIRS
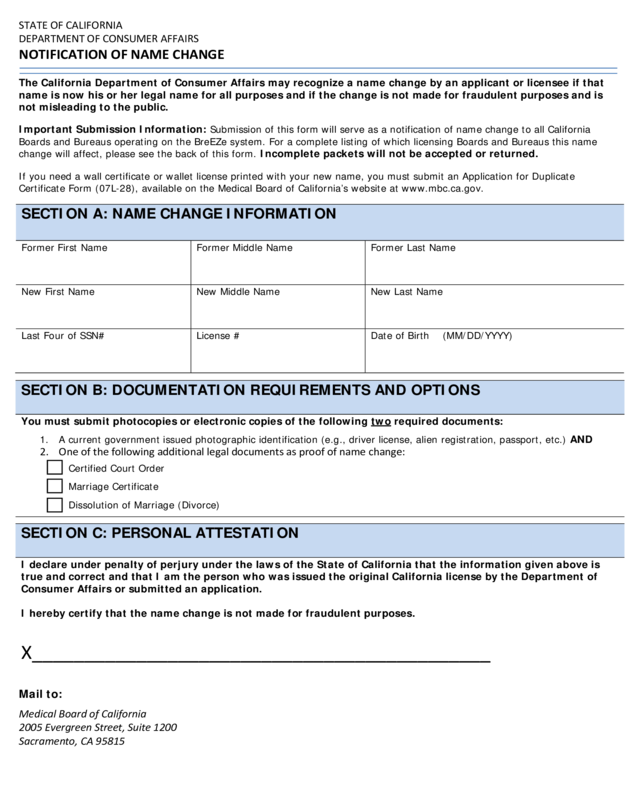
NOTIFICATION OF NAME CHANGE
The California Depa r t ment of Consu m er Affa irs may recognize a name change by an applicant or licensee if that
name is now his or her l ega l na me for all purposes and if the change is not made for fraudulent purposes and is
not misleading to the public.
Important Submission Information:
Submissio n of this form will serve as a notification of name change to all California
Boards and Bureaus operating on the BreEZe system. For a complete listing of which licensing Boards and Bureaus this name
change will affect, please see the back of this form. Incomplete packets will not be accepted or returned.
If you need a wall certificate or wallet license printed with your new name, you must submit a n Application for Duplicate
Certificate Form (07L-28), available on the Medical Board of California’s website at www.mbc.ca.gov.
Mail to:
Medical Board of California
2005 Evergreen Street, Suite 1200
Sacramento, CA 95815
SECTION A: NAME CHANGE INFORMATION
Former First Name
Former Middle Name
Former Last Name
New Fi rst Name
New Middle Name
New Last Name
Last Four of SSN#
License #
Date of Birth (MM/DD/YYYY)
SECTION B: DOCUMENTATION REQU IREMENTS AND OPTIONS
You must submit photocopies or electronic copies of the following two requ ired doc uments :
1. A current government issued photographic identification (e.g., driver license, a lien registration, passport, etc.) AND
2. One of the following additional legal documents as proof of name change:
Certified Court Order
Marriage Certificate
Dissolution of Marriage (Divorce)
SECTION C: PERSONAL ATTESTATION
I declare under penalty of perjury under the laws of the State of California that the information given above is
true and correct and that I am the person who was issued the original California lic ense by the Department of
Consumer Affairs or submitted an application.
I hereby certify that the name change is not made for fraudulent purposes.
X____________________________________________

STATE OF CALIFORNIA
DEPARTMENT OF CONSUMER AFFAIRS
NOTIFICATION OF NAME CHANGE
Boards and Bureaus this Name Change will affect:
Submission of this form will serve as a notification of na me change to all California Boards and Bureaus opera ting on the BreEZe
system. Below is a list of the licensing Boards and Bureaus currently on the BreEZe system. If you hold a license with a Board or
Bureau which is not currently on the BreEZe system, you must submit a separate name change form directly to that progr am.
• California Board of Barbering and Cosmetology
• California Board of Behavioral Sciences
• Dental Board of California
• Dental Hygiene Committee of California
• Medical Board of Calif or nia
• California Bureau of Naturopathic Medicine
• Board of Occupational Therapy
• Cal iforn ia Boar d of Optom etry
• Osteopathic Medical Board of California
• Physical Therapy Board
• Physician Assist ant Board
• Board of Podiatric Medicine
• California Board of Psychology
• Board of Re gis t er e d Nu r s in g
• Respiratory Care Board
• Bureau of Security and Investigative Services
• Veterinary Medical Board
• Board of Vocational Nursing and Psychiatric Technicians
Check this box if you hold a license with two or more of these programs
Mail to:
Medical Board of California
2005 Evergreen Street, Suite 1200
Sacramento, CA 95815


