
Fillable Printable Phs 398 (Rev. 03/16), Omb No. 0925-0001, Checklist Form Page
Fillable Printable Phs 398 (Rev. 03/16), Omb No. 0925-0001, Checklist Form Page
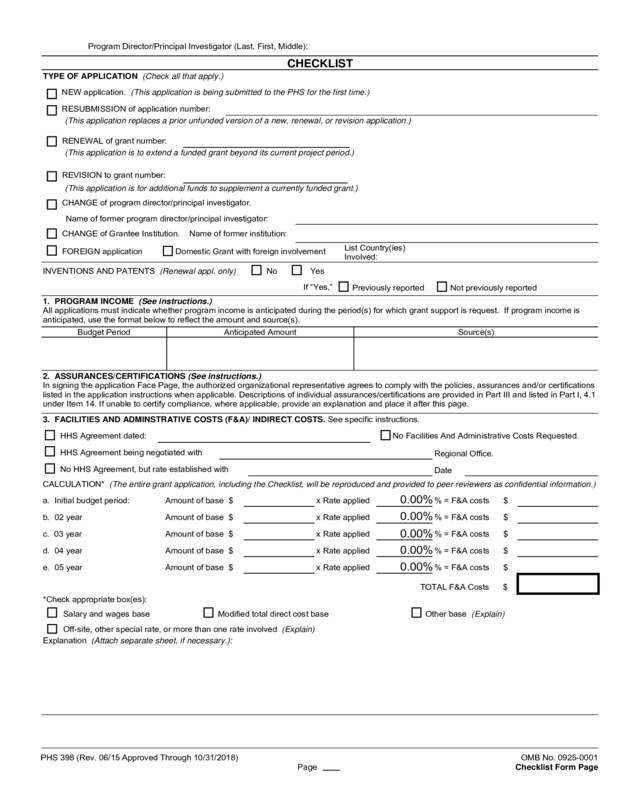
Phs 398 (Rev. 03/16), Omb No. 0925-0001, Checklist Form Page
Program Director/Principal Investigator (Last, First, Middle):
CHECKLIST
TYPE OF APPLICATION (Check all that apply.)
NEW application. (This application is being submitted to the PHS for the first time.)
RESUBMISSION of application number:
(This application replaces a prior unfunded version of a new, renewal, or revision application.)
RENEWAL of grant number:
(This application is to extend a funded grant beyond its current project period.)
REVISION to grant number:
(This application is for additional funds to supplement a currently funded grant.)
CHANGE of program director/principal investigator.
Name of former program director/principal investigator:
CHANGE of Grantee Institution. Name of former institution:
List Country(ies)
FOREIGN application Domestic Grant with foreign involvement
Involved:
INVENTIONS AND PATENTS (Renewal appl. only) No Yes
If “Yes,”
Previously reported Not previously reported
1. PROGRAM INCOME (See instructions.)
All applications must indicate whether program income is anticipated during the period(s) for which grant support is request. If program income is
anticipated, use the format below to reflect the amount and source(s).
Budget Period Anticipated Amount Source(s)
2. ASSURANCES/CERTIFICATIONS (See instructions.)
In signing the application Face Page, the authorized organizational representative agrees to comply with the policies, assurances and/or certifications
listed in the application instructions when applicable. Descriptions of individual assurances/certifications are provided in Part III and listed in Part I, 4.1
under Item 14. If unable to certify compliance, where applicable, provide an explanation and place it after this page.
3. FACILITIES AND ADMINSTRATIVE COSTS (F&A)/ INDIRECT COSTS. See specific instructions.
HHS Agreement dated: No Facilities And Administrative Costs Requested.
HHS Agreement being negotiated with
Regional Office.
No HHS Agreement, but rate established with
Date
CALCULATION* (The entire grant application, including the Checklist, will be reproduced and provided to peer reviewers as confidential information.)
a. Initial budget period: Amount of base $ x Rate applied % = F&A costs $
b. 02 year Amount of base $ x Rate applied % = F&A costs $
c. 03 year Amount of base $ x Rate applied % = F&A costs $
d. 04 year Amount of base $ x Rate applied % = F&A costs $
e. 05 year Amount of base $ x Rate applied % = F&A costs $
*Check appropriate box(es):
Salary and wages base Modified total direct cost base
TOTAL F&A Costs $
Other base (Explain)
Off-site, other special rate, or more than one rate involved (Explain)
Explanation (Attach separate sheet, if necessary.):
PHS 398 (Rev. 06/15 Approved Through 10/31/2018) OMB No. 0925-0001
Page Checklist Form Page
0.00%
0.00%
0.00%
0.00%
0.00%
Enter Rate above as a decimal (e.g., 0.25 for 25%, 0.495 for 49.5%)


