
Fillable Printable Physician Peer Feedback Form
Fillable Printable Physician Peer Feedback Form
Physician Peer Feedback Form
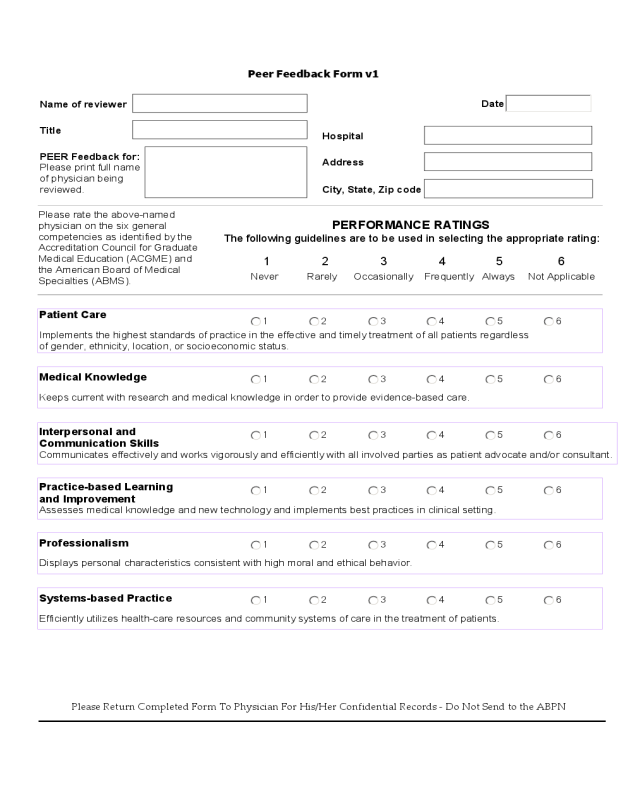
Peer Feedback Form v1
Name of reviewer
Hospital
Title
Address
PERFORMANCE RATINGS
The following guidelines are to be used in selecting the appropriate rating:
Patient Care
Implements the highest standards of practice in the effective and timely treatment of all patients regardless
of gender, ethnicity, location, or socioeconomic status.
City, State, Zip code
PEER Feedback for:
Please print full name
of physician being
reviewed.
Please rate the above-named
physician on the six general
competencies as identified by the
Accreditation Council for Graduate
Medical Education (ACGME) and
the American Board of Medical
Specialties (ABMS).
Medical Knowledge
Keeps current with research and medical knowledge in order to provide evidence-based care.
Interpersonal and
Communication Skills
Communicates effectively and works vigorously and efficiently with all involved parties as patient advocate and/or consultant.
Practice-based Learning
and Improvement
Assesses medical knowledge and new technology and implements best practices in clinical setting.
Professionalism
Displays personal characteristics consistent with high moral and ethical behavior.
Systems-based Practice
Efficiently utilizes health-care resources and community systems of care in the treatment of patients.
1 2 3 4 5 6
1 2 3 4 5 6
1 2 3 4 5 6
1 2 3 4 5 6
1 2 3 4 5 6
1 2 3 4 5 6
1 2 3 4 5 6
Never Rarely Occasionally Frequently Always
Not Applicable
Please Return Completed Form To Physician For His/Her Confidential Records - Do Not Send to the ABPN
Date


