
- Labor Certified Transcript of Payroll - Illinois
- Certified Payroll Report - Washington Department of Labor and Industries
- Certified Weekly Payroll Report - New Jersey
- Certified Transcript of Payroll - Illinois
- Public Works Payroll Reporting Form - California
- Weekly Payroll Certification for Public Works Projects - Pennsylvania
Fillable Printable Public Works Payroll Reporting Form - California
Fillable Printable Public Works Payroll Reporting Form - California
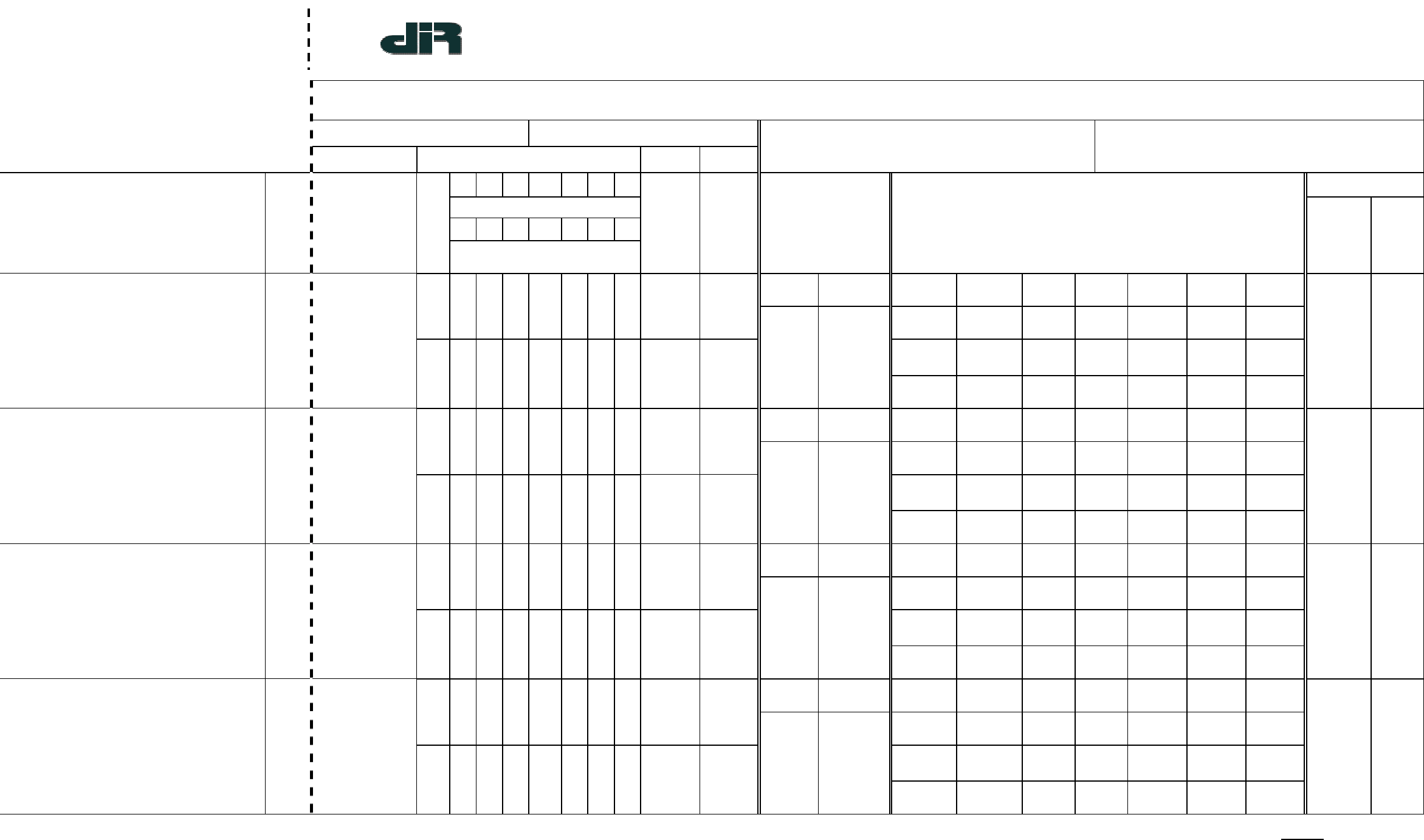
Public Works Payroll Reporting Form - California
S = STRAIGHT TIME *OTHER – Any other deductions, contributions and/or payments whether or not included or required by prevailing CERTIFICATION MUST be completed
Form A-1-131 (New 2-80) O = OVERTIME wage determinations must be separately listed. Use extra sheet(s) if necessary (See reverse side)
SDI = STATE DISABILITY INSURANCE
California
Department of
Industrial Relations
Page ______ of ______
NAME OF CONTRACTOR: CONTRACTOR'S LICENSE NO.: ADDRESS:
OR SUBCONTRACTOR: SPECIALITY LICENSE NO.:
PAYROLL NO.:
FOR WEEK ENDING:
SELF-INSURED CERTIFICATE NO.:
PROJECT OR CONTRACT NO.:
(4)
DAY
(5)
(6)
WORKERS' COMPENSATION POLICY NO.:
PROJECT AND LOCATION:
(2)
M
T
W
TH
F
S
S
(9)
DATE
(1)
NAME, ADDRESS AND
SOCIAL SECURITY NUMBER
OF EMPLOYEE
NO. OF WITH-
HOLDING
EXEMPTIONS
(3)
WORK
CLASSIFICATION
HOURS WORKED EACH DAY
TOTAL
HOURS
HOURLY
RATE
OF PAY
(7)
GROSS AMOUNT
EARNED
(8)
DEDUCTIONS, CONTRIBUTIONS AND PAYMENTS
NET WGS
PAID FOR
WEEK
CHECK
NO.
THIS
PROJECT
ALL
PROJECTS
FED.
TAX
FICA
(SOC. SEC.)
STATE
TAX
SDI
VAC/
HOLIDAY
HEALTH
& WELF.
PENSION
S
TRAING.
FUND
ADMIN
DUES
TRAV/
SUBS.
SAVINGS
OTHER*
TOTAL
DEDUC-
TIONS
O
THIS
PROJECT
ALL
PROJECTS
FED.
TAX
FICA
(SOC. SEC.)
STATE
TAX
SDI
VAC/
HOLIDAY
HEALTH
& WELF.
PENSION
S
TRAING.
FUND
ADMIN
DUES
TRAV/
SUBS.
SAVINGS
OTHER*
TOTAL
DEDUC-
TIONS
O
THIS
PROJECT
ALL
PROJECTS
FED.
TAX
FICA
(SOC. SEC.)
STATE
TAX
SDI
VAC/
HOLIDAY
HEALTH
& WELF.
PENSION
S
TRAING.
FUND
ADMIN
DUES
TRAV/
SUBS.
SAVINGS
OTHER*
TOTAL
DEDUC-
TIONS
O
THIS
PROJECT
ALL
PROJECTS
FED.
TAX
FICA
(SOC. SEC.)
STATE
TAX
SDI
VAC/
HOLIDAY
HEALTH
& WELF.
PENSION
S
TRAING.
FUND
ADMIN
DUES
TRAV/
SUBS.
SAVINGS
OTHER*
TOTAL
DEDUC-
TIONS
O
PUBLIC WORKS PAYROLL REPORTING FORM
NOTICE TO PUBLIC ENTITY
For Privacy Considerations
Fold back along dotted line prior to copying for release to general public (private persons).
(Paper Size then 8-1/2 x 11 inches)
I, , the undersigned, am the
(Name – print)
with the authority to act for and on behalf of
(Position in business)
, certify under penalty of perjury
(Name of business and/or contractor)
that the records or copies thereof submitted and consisting of
(Description, number of pages)
are the originals or true, full, and correct copies of the originals which depict the payroll record(s)
of the actual disbursements by way of cash, check, or whatever form to the individual or
individuals named.
Date: Signature:
A public entity may require a stricter and/or more extensive form of certification.


