
Fillable Printable Reduced Fee Identification Card Eligibility
Fillable Printable Reduced Fee Identification Card Eligibility
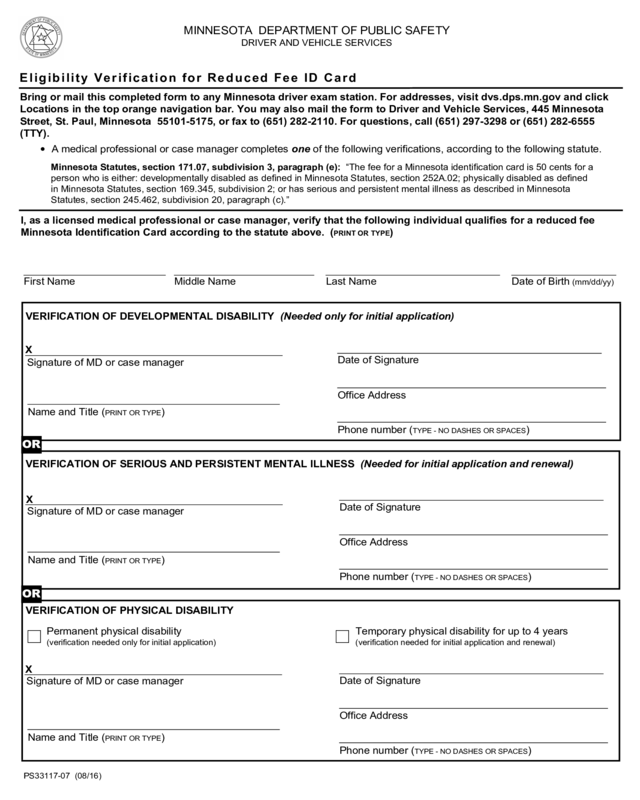
Reduced Fee Identification Card Eligibility
Minnesota Statutes, section 171.07, subdivision 3, paragraph (e): “The fee for a Minnesota identification card is 50 cents for a
person who is either: developmentally disabled as defined in Minnesota Statutes, section 252A.02; physically disabled as defined
in Minnesota Statutes, section 169.345, subdivision 2; or has serious and persistent mental illness as described in Minnesota
Statutes, section 245.462, subdivision 20, paragraph (c).”
VERIFICATION OF DEVELOPMENTAL DISABILITY (Needed only for initial application)
VERIFICATION OF SERIOUS AND PERSISTENT MENTAL ILLNESS (Needed for initial application and renewal)
VERIFICATION OF PHYSICAL DISABILITY
PS33117-07 (08/16)
Eligibility Verification for Reduced Fee ID Card
Bring or mail this completed form to any Minnesota driver exam station. For addresses, visit dvs.dps.mn.gov and click
Locations in the top orange navigation bar. You may also mail the form to Driver and Vehicle Services, 445 Minnesota
Street, St. Paul, Minnesota 55101-5175, or fax to (651) 282-2110. For questions, call (651) 297-3298 or (651) 282-6555
(TTY).
I, as a licensed medical professional or case manager, verify that the following individual qualifies for a reduced fee
Minnesota Identification Card according to the statute above. (
PRINT OR TYPE)
Date of Birth (mm/dd/yy)
Last Name Middle Name First Name
Temporary physical disability for up to 4 years
(verification needed for initial application and renewal)
Signature of MD or case manager
Signature of MD or case manager
• A medical professional or case manager completes one of the following verifications, according to the following statute.
MINNESOTA DEPARTMENT OF PUBLIC SAFETY
DRIVER AND VEHICLE SERVICES
Permanent physical disability
(verification needed only for initial application)
X
X
Office Address
Name and Title (PRINT OR TYPE)
Phone number (TYPE - NO DASHES OR SPACES)
Name and Title (PRINT OR TYPE)
Signature of MD or case manager
X
Name and Title (PRINT OR TYPE)
OR
OR
Date of Signature
Date of Signature
Office Address
Phone number (TYPE - NO DASHES OR SPACES)
Date of Signature
Office Address
Phone number (TYPE - NO DASHES OR SPACES)
Print Form


