
Fillable Printable Request for Proposal (Small Group 2-50)
Fillable Printable Request for Proposal (Small Group 2-50)
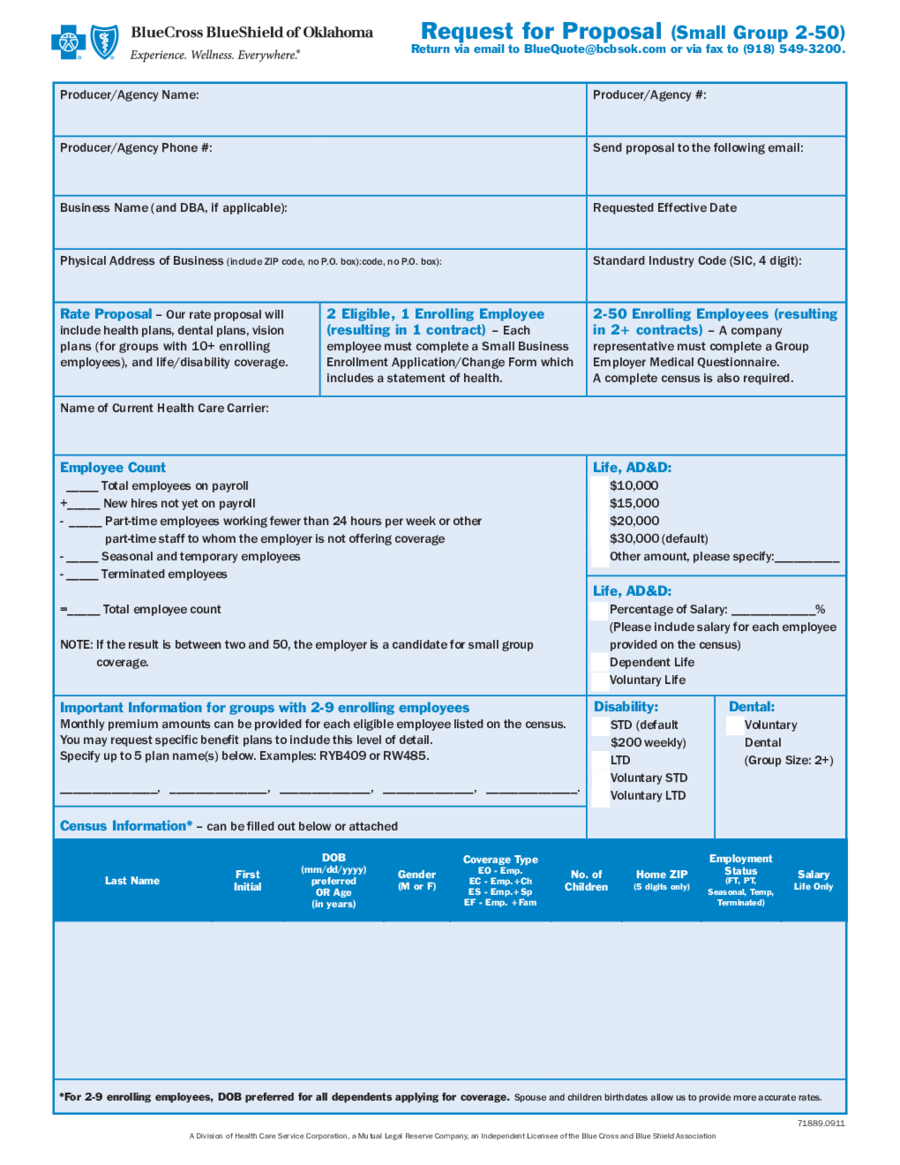
Request for Proposal (Small Group 2-50)
Request for Proposal (Small Group 2-50)
Return via email to [email protected] or via fax to (918) 549-3200.
A Division of Health Care Service Corporation, a Mutual Legal Reserve Company, an Independent Licensee of the Blue Cross and Blue Shield Association 71889.0911
A Division of Health Care Service Corporation, a Mutual Legal Reserve Company, an Independent Licensee of the Blue Cross and Blue Shield Association
Producer/Agency Name: Producer/Agency #:
Producer/Agency Phone #: Send proposal to the following email:
Business Name (and DBA, if applicable): Requested Effective Date
Physical Address of Business (include ZIP code, no P.O. box):code, no P.O. box): Standard Industry Code (SIC, 4 digit):
Rate Proposal – Our rate proposal will
include health plans, dental plans, vision
plans (for groups with 10+ enrolling
employees), and life/disability coverage.
2 Eligible, 1 Enrolling Employee
(resulting in 1 contract) – Each
employee must complete a Small Business
Enrollment Application/Change Form which
includes a statement of health.
2-50 Enrolling Employees (resulting
in 2+ contracts) – A company
representative must complete a Group
Employer Medical Questionnaire.
A complete census is also required.
Name of Current Health Care Carrier:
Employee Count
_____ Total employees on payroll
+_____ New hires not yet on payroll
- _____ Part-time employees working fewer than 24 hours per week or other
part-time staff to whom the employer is not offering coverage
- _____ Seasonal and temporary employees
- _____ Terminated employees
=_____ Total employee count
NOTE: If the result is between two and 50, the employer is a candidate for small group
coverage.
Life, AD&D:
h $10,000
h $15,000
h $20,000
h $30,000 (default)
h Other amount, please specify:__________
Life, AD&D:
h Percentage of Salary: _____________%
(Please include salary for each employee
provided on the census)
h Dependent Life
h Voluntary Life
Important Information for groups with 2-9 enrolling employees
Monthly premium amounts can be provided for each eligible employee listed on the census.
You may request specic benet plans to include this level of detail.
Specify up to 5 plan name(s) below. Examples: RYB409 or RW485.
_______________, _______________, ______________, ______________, ______________.
Census Information* – can be lled out below or attached
Last Name
First
Initial
DOB
(mm/dd/yyyy)
preferred
OR Age
(in years)
Gender
(M or F)
Coverage Type
EO - Emp.
EC - Emp.+Ch
ES - Emp.+Sp
EF - Emp. +Fam
No. of
Children
Home ZIP
(5 digits only)
Employment
Status
(FT, PT,
Seasonal, Temp,
Terminated)
Salary
Life Only
* For 2-9 enrolling employees, DOB preferred for all dependents applying for coverage. Spouse and children birthdates allow us to provide more accurate rates.
Disability:
h STD (default
$200 weekly)
h LTD
h Voluntary STD
h Voluntary LTD
Dental:
h Voluntary
Dental
(Group Size: 2+)


