
Fillable Printable Sample Blank Billing Statement
Fillable Printable Sample Blank Billing Statement
Sample Blank Billing Statement
Mailing Address:
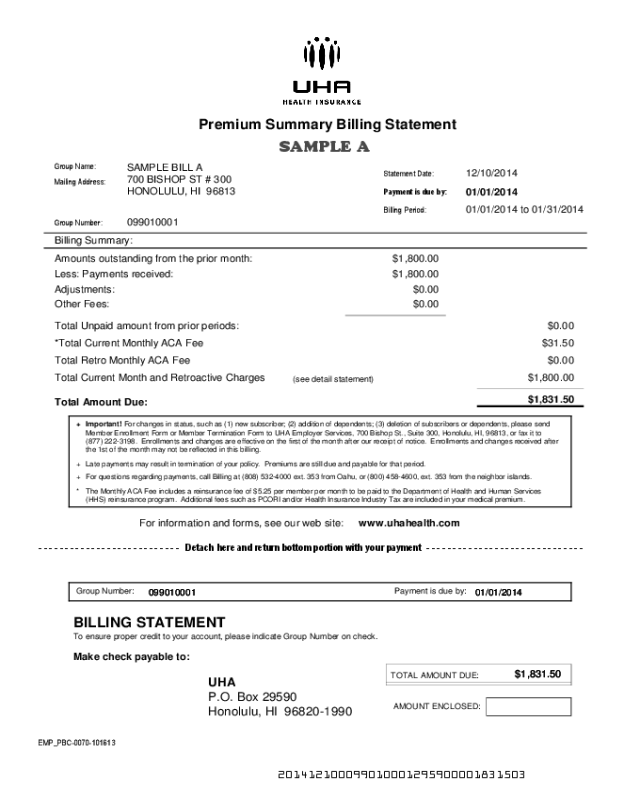
Premium Summary Billing Statement
Group Name:
Group Number:
SAMPLE BILL A
099010001
700 BISHOP ST # 300
Billing Summary:
Statement Date:
Payment is due by:
12/10/2014
Billing Period:
01/01/2014
01/01/2014 to 01/31/2014
HONOLULU, HI 96813
SAMPLE A
Amounts outstanding from the prior month:
Less: Payments received: $1,800.00
Adjustments: $0.00
Total Unpaid amount from prior periods:
Total Current Month and Retroactive Charges $1,800.00
Total Amount Due:
$1,831.50
$1,800.00
$0.00
(see detail statement)
Other Fees: $0.00
$31.50
$0.00
*Total Current Monthly ACA Fee
Total Retro Monthly ACA Fee
For changes in status, such as (1) new subscriber; (2) addition of dependents; (3) deletion of subscribers or dependents, please send
Member Enrollment Form or Member Termination Form to UHA Employer Services, 700 Bishop St., Suite 300, Honolulu, HI, 96813, or fax it to
(877) 222-3198. Enrollments and changes are effective on the first of the month after our receipt of notice. Enrollments and changes received after
the 1st of the month may not be reflected in this billing.
Late payments may result in termination of your policy. Premiums are still due and payable for that period.
For questions regarding payments, call Billing at (808) 532-4000 ext. 353 from Oahu, or (800) 458-4600, ext. 353 from the neighbor islands.
The Monthly ACA Fee includes a reinsurance fee of $5.25 per member per month to be paid to the Department of Health and Human Services
(HHS) reinsurance program. Additional fees such as PCORI and/or Health Insurance Industry Tax are included in your medical premium.
Important!
Group Number:
099010001
Payment is due by:
01/01/2014
BILLING STATEMENT
To ensure proper credit to your account, please indicate Group Number on check.
Make check payable to:
UHA
P.O. Box 29590
Honolulu, HI 96820-1990
TOTAL AMOUNT DUE:
$1,831.50
AMOUNT ENCLOSED:
For information and forms, see our web site:
www.uhahealth.com
+
+
*
+
EMP_PBC-0070-101613
201412100099010001295900001831503
- - - - - - - - - - - - - - - - - - - - - - - - - - - Detach here and return bottom portion with your payment - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
Premium Invoice
Page 1
SAMPLE A - 600
MemberID Name Med Drug Vision
HDS
Dental
ACA
Fee
Total
9901000106
Detail Premium Statement for:
Group and Division #:
Invoice Date: 12/10/2013
Current Billing Period: 01/01/2014 to 01/31/2014
Benefits: Plan 600
Contract
Type
SAMPLE BILL - A
099010001
Member
Count
SAMPLE A
SAMPLE ASAMPLE A
SAMPLE A
UHA 600 - 9901000106
Current Charges:
990100103 AFAMILY, SUBSCRIBER $915.75$120.00 $15.75$30.00$150.00$600.00F 3
990100101 ASINGLE, SUBSCRIBER $305.25$40.00 $5.25$10.00$50.00$200.00S 1
990100102 ATWOPARTY, SUBSCRIB $610.50$80.00 $10.50$20.00$100.00$400.00T 2
Subtotal: $1,200.00 $1,831.50$240.00 $31.50$60.00$300.00 6
Totals:
$1,200.00
$60.00
$300.00
Summary of Contracts
for Plan:
Single
Two Party
Family
1
1
1
UHA 600
Medical
Drug
Vision
$1,831.50
$240.00
$31.50ACA Fee
HDS Dental
Total:UHA 600
$1,200.00
$60.00
$300.00
Medical
Drug
Vision
$1,831.50
$240.00
$31.50ACA Fee
HDS DentalSummary of Contracts
for Plan(s):
Single
Two Party
Family
1
1
1
PREMIUM BILL RECONCILIATION
Terminations:
Employee Name Member ID # Termination Date Amount
( . )
( . )
.
.
Additions:
Employee Name Social Security # Effective Date Amount
Total Subtractions:
( . )
Total Additions:
.
Payment Amount Submitted:
.
Date
(Completed Enrollment Forms MUST be attached)
Changes will NOT be processed without authorized signature and date
Important:
Group Administrator Signature:
Current Billing
Period Totals:
Total Current Month and Retroactive Charges:
Note: Use this section for corrections to the Current Billing Period ONLY
For questions regarding eligibility changes, terminations, or additions, call Enrollment at
(808) 532-4007 from Oahu, or (800) 458-4600, ext. 299 from the neighbor islands.
Mailing Address:
Premium Summary Billing Statement
Group Name:
Group Number:
SAMPLE BILL B
099020002
700 BISHOP ST # 300
Billing Summary:
Statement Date:
Payment is due by:
12/10/2014
Billing Period:
01/01/2014
01/01/2014 to 01/31/2014
HONOLULU, HI 96813
SAMPLE B
Amounts outstanding from the prior month:
Less: Payments received: $1,800.00
Adjustments: $0.00
Total Unpaid amount from prior periods:
Total Current Month and Retroactive Charges $1,200.00
Total Amount Due:
$1,821.00
$2,400.00
$600.00
(see detail statement)
Other Fees: $0.00
$31.50
($10.50)
*Total Current Monthly ACA Fee
Total Retro Monthly ACA Fee
For changes in status, such as (1) new subscriber; (2) addition of dependents; (3) deletion of subscribers or dependents, please send
Member Enrollment Form or Member Termination Form to UHA Employer Services, 700 Bishop St., Suite 300, Honolulu, HI, 96813, or fax it to
(877) 222-3198. Enrollments and changes are effective on the first of the month after our receipt of notice. Enrollments and changes received after
the 1st of the month may not be reflected in this billing.
Late payments may result in termination of your policy. Premiums are still due and payable for that period.
For questions regarding payments, call Billing at (808) 532-4000 ext. 353 from Oahu, or (800) 458-4600, ext. 353 from the neighbor islands.
The Monthly ACA Fee includes a reinsurance fee of $5.25 per member per month to be paid to the Department of Health and Human Services
(HHS) reinsurance program. Additional fees such as PCORI and/or Health Insurance Industry Tax are included in your medical premium.
Important!
Group Number:
099020002
Payment is due by:
01/01/2014
BILLING STATEMENT
To ensure proper credit to your account, please indicate Group Number on check.
Make check payable to:
UHA
P.O. Box 29590
Honolulu, HI 96820-1990
TOTAL AMOUNT DUE:
$1,821.00
AMOUNT ENCLOSED:
For information and forms, see our web site:
www.uhahealth.com
+
+
*
+
EMP_PBC-0070-101613
201412100099020002295900001821004
Auto Pay
- - - - - - - - - - - - - - - - - - - - - - - - - - - Detach here and return bottom portion with your payment - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
Premium Invoice
Page 1
SAMPLE B - 3000
MemberID Name Med Drug Vision
HDS
Dental
ACA
Fee
Total
9902000203
Detail Premium Statement for:
Group and Division #:
Invoice Date: 12/10/2013
Current Billing Period: 01/01/2014 to 01/31/2014
Benefits: UHA 3000
Contract
Type
SAMPLE BILL - B
099020002
Member
Count
SAMPLE B
SAMPLE BSAMPLE B
SAMPLE B
UHA 3000 - 9902000203
Current Charges:
990200203 BFAMILY, SUBSCRIBER $915.75$120.00 $15.75$30.00$150.00$600.00F 3
990200201 BSINGLE, SUBSCRIBER $305.25$40.00 $5.25$10.00$50.00$200.00S 1
990200202 BTWOPARTY, SUBSCRIB $610.50$80.00 $10.50$20.00$100.00$400.00T 2
Subtotal: $1,200.00 $1,831.50$240.00 $31.50$60.00$300.00 6
Retro Adjustments:
990200292 ZTWOPARTY, SUBSCRIB ($610.50)($80.00) ($10.50)($20.00)($100.00)($400.00)T -2
Subtotal: ($400.00) ($610.50)($80.00) ($10.50)($20.00)($100.00) -2
Totals:
$800.00
$40.00
$200.00
Summary of Contracts
for Plan:
Single
Two Party
Family
1
1
1
UHA 3000
Medical
Drug
Vision
$1,221.00
$160.00
$21.00ACA Fee
HDS Dental
Total:UHA 3000
$800.00
$40.00
$200.00
Medical
Drug
Vision
$1,221.00
$160.00
$21.00ACA Fee
HDS DentalSummary of Contracts
for Plan(s):
Single
Two Party
Family
1
1
1
PREMIUM BILL RECONCILIATION
Terminations:
Employee Name Member ID # Termination Date Amount
( . )
( . )
.
.
Additions:
Employee Name Social Security # Effective Date Amount
Total Subtractions:
( . )
Total Additions:
.
Payment Amount Submitted:
.
Date
(Completed Enrollment Forms MUST be attached)
Changes will NOT be processed without authorized signature and date
Important:
Group Administrator Signature:
Current Billing
Period Totals:
Total Current Month and Retroactive Charges:
Note: Use this section for corrections to the Current Billing Period ONLY
For questions regarding eligibility changes, terminations, or additions, call Enrollment at
(808) 532-4007 from Oahu, or (800) 458-4600, ext. 299 from the neighbor islands.
Mailing Address:
Premium Summary Billing Statement
Group Name:
Group Number:
SAMPLE BILL C
099030003
700 BISHOP ST # 300
Billing Summary:
Statement Date:
Payment is due by:
12/10/2014
Billing Period:
01/01/2014
01/01/2014 to 01/31/2014
HONOLULU, HI 96813
SAMPLE C
Amounts outstanding from the prior month:
Less: Payments received: $2,700.00
Adjustments: $0.00
Total Unpaid amount from prior periods:
Total Current Month and Retroactive Charges $900.00
Total Amount Due:
$915.75
$2,700.00
$0.00
(see detail statement)
Other Fees: $0.00
$31.50
($15.75)
*Total Current Monthly ACA Fee
Total Retro Monthly ACA Fee
For changes in status, such as (1) new subscriber; (2) addition of dependents; (3) deletion of subscribers or dependents, please send
Member Enrollment Form or Member Termination Form to UHA Employer Services, 700 Bishop St., Suite 300, Honolulu, HI, 96813, or fax it to
(877) 222-3198. Enrollments and changes are effective on the first of the month after our receipt of notice. Enrollments and changes received after
the 1st of the month may not be reflected in this billing.
Late payments may result in termination of your policy. Premiums are still due and payable for that period.
For questions regarding payments, call Billing at (808) 532-4000 ext. 353 from Oahu, or (800) 458-4600, ext. 353 from the neighbor islands.
The Monthly ACA Fee includes a reinsurance fee of $5.25 per member per month to be paid to the Department of Health and Human Services
(HHS) reinsurance program. Additional fees such as PCORI and/or Health Insurance Industry Tax are included in your medical premium.
Important!
Group Number:
099030003
Payment is due by:
01/01/2014
BILLING STATEMENT
To ensure proper credit to your account, please indicate Group Number on check.
Make check payable to:
UHA
P.O. Box 29590
Honolulu, HI 96820-1990
TOTAL AMOUNT DUE:
$915.75
AMOUNT ENCLOSED:
For information and forms, see our web site:
www.uhahealth.com
+
+
*
+
EMP_PBC-0070-101613
201412100099030003295900000915751
- - - - - - - - - - - - - - - - - - - - - - - - - - - Detach here and return bottom portion with your payment - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
Premium Invoice
Page 1
SAMPLE C - 3000
MemberID Name Med Drug Vision
HDS
Dental
ACA
Fee
Total
9903000303
Detail Premium Statement for:
Group and Division #:
Invoice Date: 12/10/2013
Current Billing Period: 01/01/2014 to 01/31/2014
Benefits: UHA 3000
Contract
Type
SAMPLE BILL - C
099030003
Member
Count
SAMPLE C
SAMPLE CSAMPLE C
SAMPLE C
UHA 3000 - 9903000303
Current Charges:
990300303 CFAMILY, SUBSCRIBER $915.75$120.00 $15.75$30.00$150.00$600.00F 3
990300301 CSINGLE, SUBSCRIBER $305.25$40.00 $5.25$10.00$50.00$200.00S 1
990300302 CTWOPARTY, SUBSCRIB $610.50$80.00 $10.50$20.00$100.00$400.00T 2
Subtotal: $1,200.00 $1,831.50$240.00 $31.50$60.00$300.00 6
Retro Adjustments:
990300392 XFAMILY, SUBSCRIBER ($915.75)($120.00) ($15.75)($30.00)($150.00)($600.00)F -3
Subtotal: ($600.00) ($915.75)($120.00) ($15.75)($30.00)($150.00) -3
Totals:
$600.00
$30.00
$150.00
Summary of Contracts
for Plan:
Single
Two Party
Family
1
1
1
UHA 3000
Medical
Drug
Vision
$915.75
$120.00
$15.75ACA Fee
HDS Dental
Total:UHA 3000
$600.00
$30.00
$150.00
Medical
Drug
Vision
$915.75
$120.00
$15.75ACA Fee
HDS DentalSummary of Contracts
for Plan(s):
Single
Two Party
Family
1
1
1
PREMIUM BILL RECONCILIATION
Terminations:
Employee Name Member ID # Termination Date Amount
( . )
( . )
.
.
Additions:
Employee Name Social Security # Effective Date Amount
Total Subtractions:
( . )
Total Additions:
.
Payment Amount Submitted:
.
Date
(Completed Enrollment Forms MUST be attached)
Changes will NOT be processed without authorized signature and date
Important:
Group Administrator Signature:
Current Billing
Period Totals:
Total Current Month and Retroactive Charges:
Note: Use this section for corrections to the Current Billing Period ONLY
For questions regarding eligibility changes, terminations, or additions, call Enrollment at
(808) 532-4007 from Oahu, or (800) 458-4600, ext. 299 from the neighbor islands.
Mailing Address:
Premium Summary Billing Statement
Group Name:
Group Number:
SAMPLE BILL D
099040004
700 BISHOP ST # 300
Billing Summary:
Statement Date:
Payment is due by:
12/10/2014
Billing Period:
01/01/2014
01/01/2014 to 01/31/2014
HONOLULU, HI 96813
SAMPLE D
Amounts outstanding from the prior month:
Less: Payments received: $2,000.00
Adjustments: $0.00
Total Unpaid amount from prior periods:
Total Current Month and Retroactive Charges $6,000.00
Total Amount Due:
$6,189.00
$2,000.00
$0.00
(see detail statement)
Other Fees: $0.00
$126.00
$63.00
*Total Current Monthly ACA Fee
Total Retro Monthly ACA Fee
For changes in status, such as (1) new subscriber; (2) addition of dependents; (3) deletion of subscribers or dependents, please send
Member Enrollment Form or Member Termination Form to UHA Employer Services, 700 Bishop St., Suite 300, Honolulu, HI, 96813, or fax it to
(877) 222-3198. Enrollments and changes are effective on the first of the month after our receipt of notice. Enrollments and changes received after
the 1st of the month may not be reflected in this billing.
Late payments may result in termination of your policy. Premiums are still due and payable for that period.
For questions regarding payments, call Billing at (808) 532-4000 ext. 353 from Oahu, or (800) 458-4600, ext. 353 from the neighbor islands.
The Monthly ACA Fee includes a reinsurance fee of $5.25 per member per month to be paid to the Department of Health and Human Services
(HHS) reinsurance program. Additional fees such as PCORI and/or Health Insurance Industry Tax are included in your medical premium.
Important!
Group Number:
099040004
Payment is due by:
01/01/2014
BILLING STATEMENT
To ensure proper credit to your account, please indicate Group Number on check.
Make check payable to:
UHA
P.O. Box 29590
Honolulu, HI 96820-1990
TOTAL AMOUNT DUE:
$6,189.00
AMOUNT ENCLOSED:
For information and forms, see our web site:
www.uhahealth.com
+
+
*
+
EMP_PBC-0070-101613
201412100099040004295900006189005
Auto Pay
- - - - - - - - - - - - - - - - - - - - - - - - - - - Detach here and return bottom portion with your payment - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
Premium Invoice
Page 1
SAMPLE D - 3000
MemberID Name Med Drug Vision
HDS
Dental
ACA
Fee
Total
9904000403
Detail Premium Statement for:
Group and Division #:
Invoice Date: 12/10/2013
Current Billing Period: 01/01/2014 to 01/31/2014
Benefits: UHA 3000
Contract
Type
SAMPLE BILL - D
099040004
Member
Count
SAMPLE D
SAMPLE DSAMPLE D
SAMPLE D
UHA 3000 - 9904000403
Current Charges:
990400412 FAMILY2, G SUB2000 $515.75$0.00 $15.75$30.00$120.00$350.00F 3
990400409 NEWFAMILY2, K SUB2000 $515.75$0.00 $15.75$30.00$120.00$350.00F 3
990400410 NEWSINGLE2, L SUB2000 $205.25$0.00 $5.25$10.00$40.00$150.00S 1
990400411 NEWTWOP2, M SUB2000 $310.50$0.00 $10.50$20.00$80.00$200.00T 2
990400407 SINGLE2, H SUB2000 $205.25$0.00 $5.25$10.00$40.00$150.00S 1
990400408 TWOPARTY2, J SUB2000 $310.50$0.00 $10.50$20.00$80.00$200.00T 2
Subtotal: $1,400.00 $2,063.00$0.00 $63.00$120.00$480.00 12
Retro Adjustments:
990400412 NEWFAMILY2, K SUB2000 $515.75$0.00 $15.75$30.00$120.00$350.00F 3
990400410 NEWSINGLE2, L SUB2000 $205.25$0.00 $5.25$10.00$40.00$150.00S 1
990400411 NEWTWOP2, M SUB2000 $310.50$0.00 $10.50$20.00$80.00$200.00T 2
Subtotal: $700.00 $1,031.50$0.00 $31.50$60.00$240.00 6
Totals:
$2,100.00
$180.00
$720.00
Summary of Contracts
for Plan:
Single
Two Party
Family
2
2
2
UHA 3000
Medical
Drug
Vision
$3,094.50
$0.00
$94.50ACA Fee
HDS Dental
Total:UHA 3000
UHA 600 - 9904000406
Current Charges:
990400403 FAMILY6, A SUB600 $515.75$0.00 $15.75$30.00$120.00$350.00F 3
990400406 NEWFAMILY6, D SUB600 $515.75$0.00 $15.75$30.00$120.00$350.00F 3
990400404 NEWSINGLE6, E SUB600 $205.25$0.00 $5.25$10.00$40.00$150.00S 1
990400405 NEWTWOP6, F SUB600 $310.50$0.00 $10.50$20.00$80.00$200.00T 2
990400401 SINGLE6, B SUB600 $205.25$0.00 $5.25$10.00$40.00$150.00S 1
990400402 TWOPARTY6, C SUB600 $310.50$0.00 $10.50$20.00$80.00$200.00T 2
Subtotal: $1,400.00 $2,063.00$0.00 $63.00$120.00$480.00 12
Retro Adjustments:
990400406 NEWFAMILY6, D SUB600 $515.75$0.00 $15.75$30.00$120.00$350.00F 3
990400404 NEWSINGLE6, E SUB600 $205.25$0.00 $5.25$10.00$40.00$150.00S 1
990400405 NEWTWOP6, F SUB600 $310.50$0.00 $10.50$20.00$80.00$200.00T 2
Subtotal: $700.00 $1,031.50$0.00 $31.50$60.00$240.00 6
Premium Invoice
Page 2
SAMPLE D - 600
MemberID Name Med Drug Vision
HDS
Dental
ACA
Fee
Total
9904000406
Detail Premium Statement for:
Group and Division #:
Invoice Date: 12/10/2013
Current Billing Period: 01/01/2014 to 01/31/2014
Benefits: Plan 600
Contract
Type
SAMPLE BILL - D
099040004
Member
Count
SAMPLE D
SAMPLE DSAMPLE D
SAMPLE D
Totals:
$2,100.00
$180.00
$720.00
Summary of Contracts
for Plan:
Single
Two Party
Family
2
2
2
UHA 600
Medical
Drug
Vision
$3,094.50
$0.00
$94.50ACA Fee
HDS Dental
Total:UHA 600
$4,200.00
$360.00
$1,440.00
Medical
Drug
Vision
$6,189.00
$0.00
$189.00ACA Fee
HDS DentalSummary of Contracts
for Plan(s):
Single
Two Party
Family
4
4
4
PREMIUM BILL RECONCILIATION
Terminations:
Employee Name Member ID # Termination Date Amount
( . )
( . )
.
.
Additions:
Employee Name Social Security # Effective Date Amount
Total Subtractions:
( . )
Total Additions:
.
Payment Amount Submitted:
.
Date
(Completed Enrollment Forms MUST be attached)
Changes will NOT be processed without authorized signature and date
Important:
Group Administrator Signature:
Current Billing
Period Totals:
Total Current Month and Retroactive Charges:
Note: Use this section for corrections to the Current Billing Period ONLY
For questions regarding eligibility changes, terminations, or additions, call Enrollment at
(808) 532-4007 from Oahu, or (800) 458-4600, ext. 299 from the neighbor islands.


