
Fillable Printable Sf2820
Fillable Printable Sf2820
Sf2820
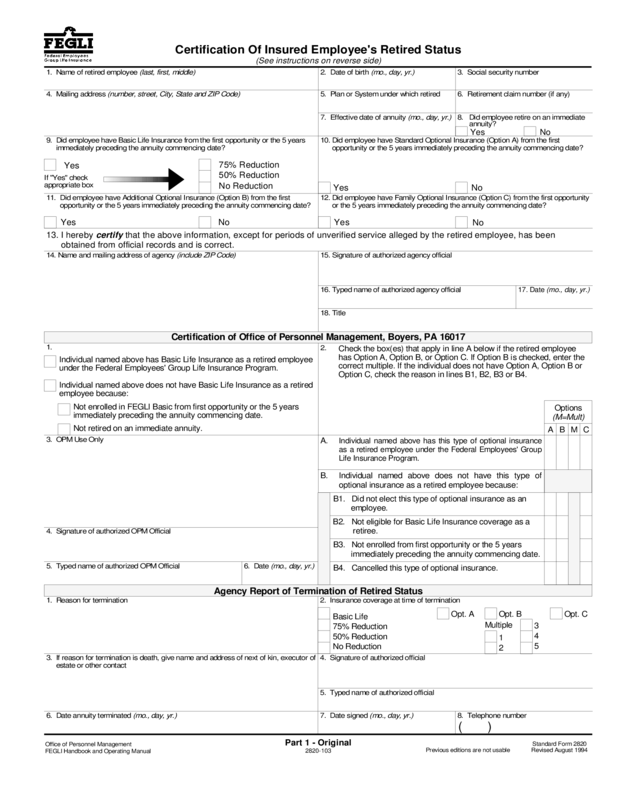
Certification Of Insured Employee's Retired Status
(See ins truct ions on reverse side)
2820-103
Offic e of Personnel Management
FEGLI Handbook and Operating Manual
Part 1 - Original
1. N ame of retired em plo yee
(last, first, middle)
8. D id employee retire on an immediate
annuity?
7. Effectiv e date of annu ity
(mo ., day , yr.)
6. R etirement claim nu m b er (if any)5. Plan or S ystem un der which retired
3 . So c ia l s e c u r ity n um b er2. Date o f birth
(mo ., da y, yr .)
4. Ma iling ad dress
(num be r, street, City, S tate an d Z IP C ode)
9. D id em ploy ee have B asic Life Insu rance from the first opportunity or the 5 y ears
im mediately p receding the an nuity com mencing da te?
10. D id em ploye e h ave Standard Option al Insu rance (O ption A) from the first
oppo rtunity or the 5 y ears immediately p receding the ann uity com m e ncing da te?
75% Reduction
50% Reduction
No Reduction
13. I hereby
certify
that the above information, except for periods of unverified service alleged by the retired employee, has been
obtained from official records and is correct.
Agency Report of Termination of Retired Status
Certification of Office of Personnel Management, Boyers, PA 16017
11. D id em p loyee have A dd itional Optional Insurance (O p tion B) from the first
opportunity or the 5 y e ars imm e diately preced ing the a nnuity com m en cing d ate?
12. D id em ploye e h ave F a m ily Optional Insuranc e (O ption C) from the first opp ortunity
or the 5 y ears immediately p receding the ann uity com mencing da te?
14. N ame and mailing address of agenc y
(include ZIP Co de)
15. Signature of autho rized agency official
16. Typed name of au thorized ag ency o fficial
18. Title
1 7. Date
(mo., day, yr.)
Individual named above has this type of optional insurance
as a retired empl oyee under the Federal Employees' Group
Life Insurance P rogra m .
Individual named above does not have this type of
optional insurance as a retired employee because:
B3. Not enrolled from first opportunity or the 5 years
immediately preceding the annuity com mencing date.
B4. Cancelled this type of optional insurance.
3. OPM Use Only
6 . Da te
(mo. , d ay, yr.)
6. Da te an nuity termina ted
(mo ., day , yr.)
1. R easo n for termination
3. If reason for term ination is d eath, give nam e a nd address of next of kin, e xecutor of
es tate or other c on tact
4. Signature of a uthorized official
7. Da te signed
(mo., day, yr.)
No
Yes
Yes
No
No
Individu al na m ed above has Basic Life Insurance as a retired employee
under the Federal Employees' Gro up Life Insurance Progr am .
Individual named above does not have Basic Life Insurance as a retired
emp loyee because:
Not enrolled in FEGLI Basic from first opportunity or the 5 years
imme diately prece ding the annuity com m encing date.
Not retired on a n immediate annuity.
5. Typed name of a uthorize d O PM O fficial
2. Insurance cov erage at time o f termination
Op t. A Op t. B Op t. C
1
2
3
4
5
5. Typed name of authorized official
Multiple
Yes No
Basic Life
75% R eduction
50% R eduction
No Reduction
8. Telephone number
( )
1.
4. Signature of authorized O PM O fficial
Yes
Yes
If "Yes" ch eck
approp riate bo x
B1. Did not elect this type of optional insuranc e as an
employee.
B2. Not e ligible for Basic L ife Insurance cove rage a s a
re tiree.
Options
(M=Mult)
ABMC
2.
A.
B.
Check the box(es ) that app ly in line A be low if the retired employee
has Optio n A, Option B , or Option C . If Option B is checked , e nter t h e
correct multiple. If the individual does not h ave O ption A, Option B or
Op tion C , chec k the re ason in lines B1 , B2, B 3 or B4 .
Standard Form 2820
Previous editions are not usable Revised August 1994
Instructions to Agency or Office Administering the Retirement System
Completion of Certification
- Prepare thi s cert if i cat ion f or each insured employee who has reti r ed under any Feder al
syst em ot her t han t he Civ i l Serv ice Reti rement System or Feder al Employees' Reti rement System and who submits a
com pleted A gency Certification of Insurance Status (SF 282 1).
Disposition of Certification
- Send Part 1 and Pa rt 2 of thi s certi fi cat ion and al l li fe i nsurance electi on forms together
with SF 2821 to the Office of Personnel Management, Boyers, PA 16017. Retain Part 3 in your file. Part 2 will be
returned for your reco rds indicating whether the retired employee is insured.
Immediate Annuity
- Referred to in item 8, m eans one which begins to a ccrue not later than 1 month following the date
that the insura nce would otherwise cease. (This date is shown in item 6 of the Agency Certification of Insu rance Status
[SF 2821], subm itted to you by the retiring em ployee.)
Reduction or Cancellation of Optional Insurance
- An annuitant under ag e 65 desiring to reduce or cancel his or her
optional insur ance should be i nstructed t o s ubmit a SF 2817 reduci ng or decli ni ng (c ancel i ng) t he opti onal ins urance t o
his or her retirement syst em so deductions can be stopped. The reti r ement system should send the original of t he form
to the Office of Personnel Managem ent and retain Part 2.
Changing Post-Retirement Basic Life Insurance to 75% Reduction
- An annuit ant who wants t o change his or her
Basic Life Insurance from No Reduction or 50% Reduction to the 75% Reduction may do so at any time. The change is
effective at the beginning of the month following the m onth in which the request is received.
Reporting Terminations of A nnuity
- Upon death of an insured annuitant or upon termination of an annuity, com plete
the appropriat e box on Par t 2 of the SF 2820 and s end i t to t he Off i c e of Personnel Manageme nt, Boyers, PA 16017. If
you are in contact with the family of a deceased annuitan t and obtain a completed claim for death benefits (Form FE-6),
it shoul d be sent to t he Off ice of Personnel Management t ogether wi th Part 2 of t he SF 2820 and other document s t o
support the claim.
Reverse of Standard Form 2820
Revised August 1994
Certification Of Insured Employee's Retired Status
(See i nstructions on reverse side)
2820-103
Standard Form 2820
Previous editio ns ar e not usable Revised August 1994
Office of Personnel Management
FEGLI H andbook and Operating Manual
Part 2 - Duplicate To Be Returned To A gency
1. Na m e of retired employee
(la st, firs t, mid d le )
8. Did em p loyee retire on an im m e diate
annuity?
7 . Effe c tive date of a n nuity
(mo ., day , yr.)
6. R etireme nt claim nu m be r (if any)5. Plan or System under which retired
3. So cial sec urity number2. D ate of birth
(mo ., day , yr.)
4. Mailing address
(n umber, street, C ity, State and ZIP Code)
9. D id em ploye e h ave B a sic Life Insuran ce from the first opportunity or the 5 years
imm edia tely preceding the ann uity com m e ncing date?
10. Did employe e ha ve S tand ard O p tional Insuran ce (O ption A) from the first
opportunity or the 5 years immediately prece ding the a nn uity comme ncing date?
75% Reduction
50% Reduction
No Reducti on
13. I hereby
certify
that the above information, except for periods of unverified service alleged by the retired employee, has been
obtained from official records and is correct.
Agency Report of Termination of Retired Status
Certification of Office of Personnel M anageme nt, Boye rs, PA 16017
11. D id em p loyee have A dditional Op tional Insuran ce (O ption B) from the first
oppo rtunity o r the 5 yea rs imm e diately p receding the an nuity com mencing da te?
12. Did employe e ha ve F amily O ptional Insu rance (O p tion C ) from the first o ppo rtunity
or the 5 y ears immediately prece ding the ann uity com m e nc ing date?
14. N ame and mailing a ddress o f agenc y
(include ZIP C od e)
15. S ignature of authorized age ncy official
16. Typed name of authorized age ncy official
1 8 . Title
1 7. Da te
(mo., day, yr.)
Individual named above has this type of optional insurance
as a retired employee under the Federal Employees' Group
Life Insurance Program.
Individual named above does not have this type of
optional insurance as a r etired employee because:
3. OPM Use Only
6. Da te
(mo., day, yr.)
6. Date annuity terminated
(mo. , d ay, yr.)
1. Re ason for termination
3. If reason for termination is de ath, give name and ad dress o f nex t of k in, exe cutor of
es tate or o ther c o ntact
4. Signature of authorized official
7. Date signed
(mo ., da y, yr .)
No
Yes
Yes
No
No
Individual named above h as B asic Life Insurance a s a r etired employee
under the Federal Employee s' Grou p Life Insurance Progra m .
Individual named above d oes not have Basic Life Insurance as a retired
employ ee because:
Not enrolled in FE G LI B asic from first o ppor tunity or the 5 ye ars
im m ediately preceding the annuity commencing date.
Not retired on an im mediate annuity.
5. Typed name of authorized O PM O fficial
2. In sura n ce c o v erage at tim e of te r min a tio n
Opt. A Op t. B Op t. C
1
2
3
4
5
5. Typed name of authorized official
Multiple
Yes No
Basic Life
75% Reduction
50% Reduction
No Reduction
8. Teleph one number
( )
1.
4. Signature of autho rized O PM O fficial
Yes
Yes
If "Ye s " ch eck
appropriate box
B3. Not enrolled from first o pportunity or the 5 years
immediately preceding the an nuity com m encing d ate.
B4. Cancelled this type of op tional insurance.
B1. Did not elect this typ e of optional insurance as an
employee.
B 2 . Not eligible for Basic L ife Insura nce c o v erage as a
retire e .
Options
(M=Mult)
ABMC
A.
B.
2.
Check the box(es ) that app ly in line A be low if the retired employee
has Optio n A, Option B , or Option C . If Option B is checked , e nter t h e
correct multiple. If the individual does not h ave O ption A, Option B or
Op tion C , chec k the re ason in lines B1 , B2, B 3 or B4 .
Instructions to Agency or Office Administering the Retirement System
Completion of Certification
- Prepare thi s cert if i cat ion f or each insured employee who has reti r ed under any Feder al
syst em ot her t han t he Civ i l Serv ice Reti rement System or Feder al Employees' Reti rement System and who submits a
com pleted A gency Certification of Insurance Status (SF 282 1).
Disposition of Certification
- Send Part 1 and Pa rt 2 of thi s certi fi cat ion and al l li fe i nsurance electi on forms together
with SF 2821 to the Office of Personnel Management, Boyers, PA 16017. Retain Part 3 in your file. Part 2 will be
returned for your reco rds indicating whether the retired employee is insured.
Immediate Annuity
- Referred to in item 8, m eans one which begins to a ccrue not later than 1 month following the date
that the insura nce would otherwise cease. (This date is shown in item 6 of the Agency Certification of Insu rance Status
[SF 2821], subm itted to you by the retiring em ployee.)
Reduction or Cancellation of Optional Insurance
- An annuitant under ag e 65 desiring to reduce or cancel his or her
optional insur ance should be i nstructed t o s ubmit a SF 2817 reduci ng or decli ni ng (c ancel i ng) t he opti onal ins urance t o
his or her retirement syst em so deductions can be stopped. The reti r ement system should send the original of t he form
to the Office of Personnel Managem ent and retain Part 2.
Changing Post-Retirement Basic Life Insurance to 75% Reduction
- An annuit ant who wants t o change his or her
Basic Life Insurance from No Reduction or 50% Reduction to the 75% Reduction may do so at any time. The change is
effective at the beginning of the month following the m onth in which the request is received.
Reporting Terminations of A nnuity
- Upon death of an insured annuitant or upon termination of an annuity, com plete
the appropriat e box on Par t 2 of the SF 2820 and s end i t to t he Off i c e of Personnel Manageme nt, Boyers, PA 16017. If
you are in contact with the family of a deceased annuitan t and obtain a completed claim for death benefits (Form FE-6),
it shoul d be sent to t he Off ice of Personnel Management t ogether wi th Part 2 of t he SF 2820 and other document s t o
support the claim.
Reverse of Standard Form 2820
Revised August 1994
Certification Of Insured Employee's Retired Status
(See i nstructions on reverse side)
2820-103
Standard Form 2820
Previous editio ns ar e not usable Revised August 1994
Office of Personnel Management
FEGLI H andbook and Operating Manual
Part 3 - File C opy
1. Na m e of retired employee
(la st, firs t, mid d le )
8. Did em p loyee retire on an im m e diate
annuity?
7 . Effe c tive date of a n nuity
(mo ., day , yr.)
6. R etireme nt claim nu m be r (if any)5. Plan or System under which retired
3. So cial sec urity number2. D ate of birth
(mo ., day , yr.)
4. Mailing address
(n umber, street, C ity, State and ZIP Code)
9. D id em ploye e h ave B a sic Life Insuran ce from the first opportunity or the 5 years
imm edia tely preceding the ann uity com m e ncing date?
10. Did employe e ha ve S tand ard O p tional Insuran ce (O ption A) from the first
opportunity or the 5 years immediately prece ding the a nn uity comme ncing date?
75% Reduction
50% Reduction
No Reducti on
13. I hereby
certify
that the above information, except for periods of unverified service alleged by the retired employee, has been
obtained from official records and is correct.
Agency Report of Termination of Retired Status
Certification of Office of Personnel M anageme nt, Boye rs, PA 16017
11. D id em p loyee have A dditional Op tional Insuran ce (O ption B) from the first
oppo rtunity o r the 5 yea rs imm e diately p receding the an nuity com mencing da te?
12. Did employe e ha ve F amily O ptional Insu rance (O p tion C ) from the first o ppo rtunity
or the 5 y ears immediately prece ding the ann uity com m e nc ing date?
14. N ame and mailing a ddress o f agenc y
(include ZIP C od e)
15. S ignature of authorized age ncy official
16. Typed name of authorized age ncy official
1 8 . Title
1 7. Da te
(mo., day, yr.)
Check the box(es ) that app ly in line A be low if the retired employee
has Optio n A, Option B , or Option C . If Option B is checked , e nter t h e
correct multiple. If the individual does not h ave O ption A, Option B or
Op tion C , chec k the re ason in lines B1 , B2, B 3 or B4 .
Individual named above has this type of optional insurance
as a retired employee under the Federal Employees' Group
Life Insurance Program.
Individual named above does not have this type of
optional insurance as a r etired employee because:
3. OPM Use Only
6. Da te
(mo., day, yr.)
6. Date annuity terminated
(mo. , d ay, yr.)
1. Re ason for termination
3. If reason for termination is de ath, give name and ad dress o f nex t of k in, exe cutor of
es tate or o ther c o ntact
4. Signature of authorized official
7. Date signed
(mo ., da y, yr .)
No
Yes
Yes
No
No
Individual named above h as B asic Life Insurance a s a r etired employee
under the Federal Employee s' Grou p Life Insurance Progra m .
Individual named above d oes not have Basic Life Insurance as a retired
employ ee because:
Not enrolled in FE G LI B asic from first o ppor tunity or the 5 ye ars
im m ediately preceding the annuity commencing date.
Not retired on an im mediate annuity.
5. Typed name of authorized O PM O fficial
2. In sura n ce c o v erage at tim e of te r min a tio n
Opt. A Op t. B Op t. C
1
2
3
4
5
5. Typed name of authorized official
Multiple
Yes No
Basic Life
75% Reduction
50% Reduction
No Reduction
8. Teleph one number
( )
1.
4. Signature of autho rized O PM O fficial
Yes
Yes
If "Ye s " ch eck
appropriate box
B3. Not enrolled from first opportunity or the 5 years
immediately preceding the annuity com mencing date.
B4. Cancelled this type of optional insurance.
B1. Did not elect this type of optional insuranc e as an
employee.
B2. Not e ligible for Basic L ife Insurance cove rage a s a
re tiree.
Options
(M=Mult)
AB
M
C
A.
B.
2.
Instructions to Agency or Office Administering the Retirement System
Completion of Certification
- Prepare this cert if ic ati on for each insur ed empl oye e who has r etir ed under any Federal
system ot her t han the Civi l Service Ret ir ement System or Feder al Employees' Reti rement System and who submit s a
completed Agency Certification of Insurance Status (SF 2821).
Disposition of Certification
- Send Part 1 a nd Part 2 of thi s c ertif i c ati on and all li fe i ns ur an ce el ec ti on f or ms t oget her
with SF 2821 to the Office of Personnel Management, Boyers, PA 16017. Retain Part 3 in your file. Part 2 will be
re turned for your records indicating whether the retired employee is insured.
Immediate Annuity
- Referred to in item 8, means one which begins to accrue not later than 1 month follow ing the date
t hat the i ns uranc e would ot herwise cease. (Thi s dat e i s shown in it em 6 of the Agency Cert i fi cat ion of Insurance Status
[SF 2821], submitted to you by the retiring em ployee.)
Reduction or Cancellati on of Optional I nsurance
- An annuitant under age 65 desiring to reduce or cancel his or her
optional i ns urance should be i nstr uct ed t o submit a SF 2817 reducing or decl i ning (cancel i ng) the opt i onal i ns urance to
his or her r et i rement system so deductions can be stopped. The retirement system should send the ori gi nal of the form
to the Office of Personn el Managem ent and retain Part 2.
Changing Post-Retirement Basic Life Insurance to 75% Reduction
- An annui t ant who wants t o change hi s or her
Basic Life Insurance from No Reduction or 50% Reduction to the 75% Reduction may do so at any time. The change is
effective at the beginning of the month following the month in which the request is received.
Reporting Terminations of Annuity
- Upon death of an insured annuitant or upon termination of an annuity, complete
t he appropri at e box on Par t 2 of the SF 2820 and send it t o the Offi c e of Personnel Management, Boyers, PA 16017. If
you are in contact with the family of a deceased annuitant and obtain a completed claim for death benefits (Form F E -6),
it shoul d be sent to t he Off ice of Personnel Management t ogether wit h Part 2 of t he SF 2820 and other documents t o
support the claim.
Reverse of Standard Form 2820
Revised August 1994


