
Fillable Printable Standard Form 91
Fillable Printable Standard Form 91
Standard Form 91
NSN 7540-00-634-4041
Previous edition not usable
STANDARD FORM 91 (2/2004)
Prescribed by GSA-FMR 102-34.295
MOTOR VEHICLE
ACCIDENT REPORT
Please read the
Privacy Act State-
ment on Page 3
INSTRUCTIONS: Sections I through IX are filled out by the vehicle operator. Section X,
items 73 thru 83c are filled on by the operator's supervisor. Section XI thru XIII are filled out
by an accident investigator for bodily injury, fatality,and/or damage exceeding $500.
SECTION I - FEDERAL VEHICLE DATA
DATE OF ACCIDENT
2. DRIVER'S LICENSE NO./STATE/LIMITATIONS
1. DRIVER'S NAME (Last, first, middle)
4a. DEPARTMENT/FEDERAL AGENCY PERMANENT OFFICE ADDRESS 4b. WORK TELEPHONE NUMBER
5. TAG OR IDENTIFICATION NUMBER 6. EST. REPAIR COST 7. YEAR OF VEHICLE 8. MAKE 9. MODEL 10. SEAT BELTS USED
11. DESCRIBE VEHICLE DAMAGE
SECTION II - OTHER VEHICLE DATA (Use Section VIII if additional space is needed)
12. DRIVER'S NAME (Last, first, middle) 13. SOCIAL SECURITY NO./
TAX IDENTIFICATION NO.
14. DRIVER'S LICENSE NO./STATE/LIMITATIONS
15. a DRIVER'S WORK ADDRESS 15b. WORK TELEPHONE NUMBER
16a. DRIVER'SHOME ADDRESS 16b. HOME TELEPHONE NUMBER
17. DESCRIPTION OF VEHICLE DAMAGE 18. ESTIMATED REPAIR COST
19. YEAR OF VEHICLE 20. MAKE OF VEHICLE 21. MODEL OF VEHICLE 22. TAG NUMBER AND STATE
23a. DRIVE'S INSURANCE COMPANY NAME AND ADDRESS
24. VEHICLE IS 25a. OWNER'S NAME(S) (Last, first, middle)
23b. POLICY NUMBER
23c. TELEPHONE NUMBER
25b. TELEPHONE NUMBER
CO-OWNED
LEASED
RENTAL
PRIVATELY OWNED
SECTION III - KILLED OR INJURED (Use Section VIII if additional space is needed)
A
B
27. NAME (last, first, middle) 28. SEX 29. DATE OF BIRTH
30. ADDRESS
31. MARK "X" IN TWO APPROPRIATE BOXES 32. IN WHICH VEHICLE 33. LOCATION IN VEHICLE 34. FIRST AID GIVEN BY
35. TRANSPORTED BY 36. TRANSPORTED TO
37. NAME (last, first, middle) 38. SEX 39. DATE OF BIRTH
44. FIRST AID GIVEN BY
43. LOCATION IN VEHICLE
42. IN WHICH VEHICLE
41. MARK "X" IN TWO APPROPRIATE BOXES
46. TRANSPORTED TO45. TRANSPORTED BY
40. ADDRESS
47. Pedes-
trian
a. NAME OF STREET OR HIGHWAY
FROM
TO
b. DIRECTION OF PEDESTRIAN (SW corner to NW corner, etc.)
c. DESCRIBE WHAT PEDESTRIAN WAS DOING AT TIME OF ACCIDENT (crossing intersection with signal, against signal, diagonally; in roadway playing,
walking, hitchhiking, etc.)
YES NO
KILLED
KILLED
INJURED
INJURED
DRIVER
DRIVER
HELPER
HELPER
PASSENGER
PASSENGER
PEDESTRIAN
PEDESTRIAN
FED
FED
OTHER (2)
OTHER (2)
26. OWNER'S ADDRESS(ES)
$
$
STANDARD FORM 91 (2/2004) PAGE 2
SECTION IV - ACCIDENT TIME AND LOCATION (Use section VII if additional space is needed.)
48. DATE OF ACCIDENT 49. PLACE OF ACCIDENT (Street address, city, state, ZIP Code; Nearest landmark; Distance nearest intersection; Kind of locality (industrial, business,
residential, open country, etc.); Road description).
50. TIME OF ACCIDENT
AM
PM
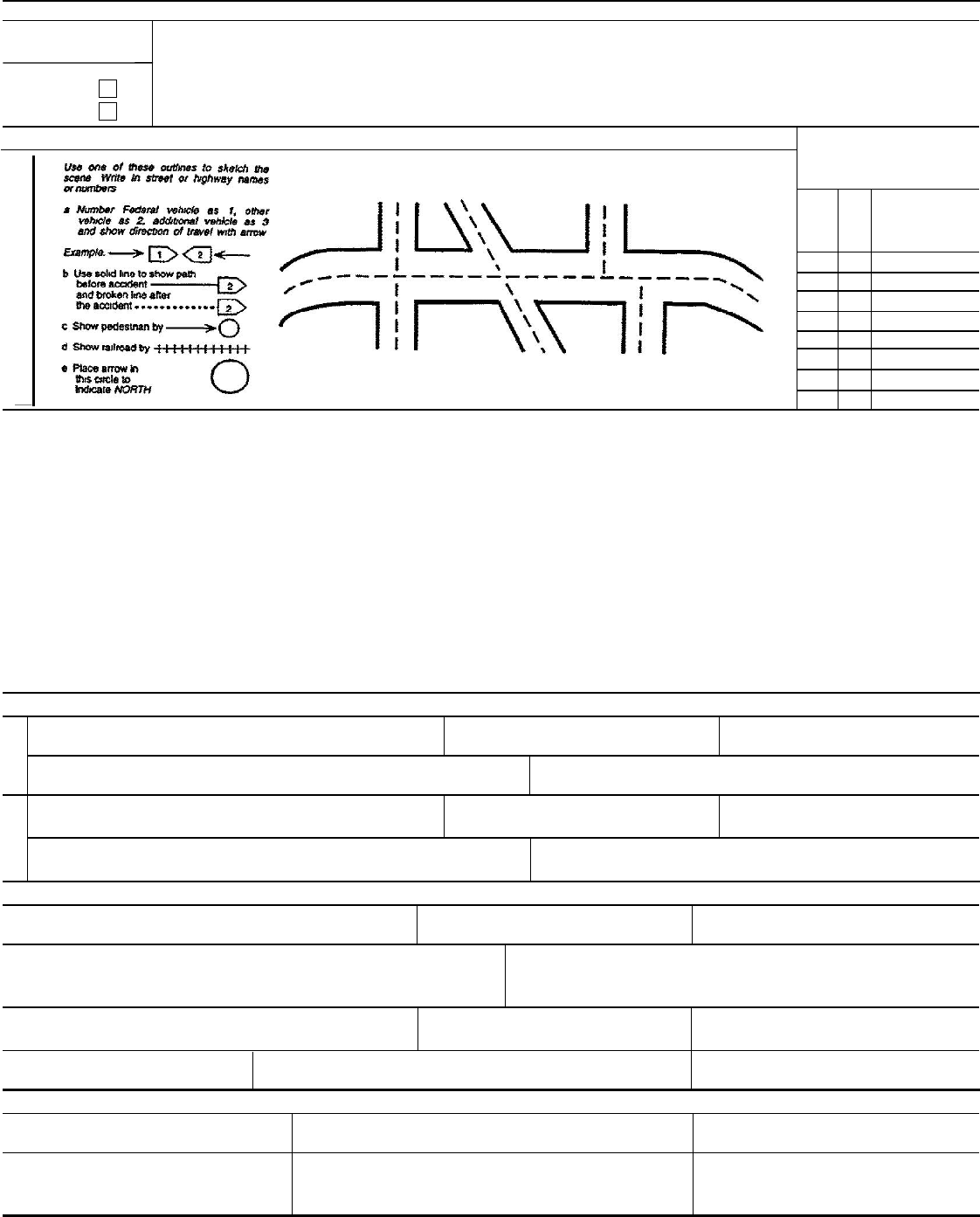
51. INDICATE ON THIS DIAGRAM HOW THE ACCIDENT HAPPENED
52. POINT OF IMPACT
(Check one for each
vehicle)
FED 2 AREA
a. Front
b. R. Front
c. L. Front
d. Rear
e. R. Rear
f. L. Rear
g. R. Side
h. L. Side
53. DESCRIBE WHAT HAPPENED (Refer to vehicles as "Fed", "2", "3", etc. Please include information on posted speed limit, approximate speed of vehicles, road conditions,
weather conditions, weather conditions, driver visibility, condition of accident vehicles, traffic controls (warning light, stop signal,etc.), condition of light (daylight, dusk, night,
dawn, artificial light, etc.), and driver actions (making a U-turn, passing, stopped in traffic, etc.)
SECTION V - WITNESS/PASSENGER (Witness must fill out SF 94, Statement of Witness) (Continue in Section VIII.)
A
B
54. NAME (Last, first, middle) 55. WORK TELEPHONE NUMBER 56. HOME TELEPHONE NUMBER
57. WORK ADDRESS 58. HOME ADDRESS
63. HOME ADDRESS62. WORK ADDRESS
61. HOME TELEPHONE NUMBER60. WORK TELEPHONE NUMBER59. NAME (Last, first, middle)
SECTION VI - PROPERTY DAMAGE (Use Section VIII if additional space is needed.)
64a. NAME OF OWNER (Last, first, middle) 64b. WORK TELEPHONE NUMBER 64c. HOME TELEPHONE NUMBER
64d. WORK ADDRESS 64e. HOME ADDRESS
65a. NAME OF INSURANCE COMPANY 65b. TELEPHONE NUMBER 65c. POLICY NUMBER
66. ITEM DAMAGED 67. LOCATION OF DAMAGED ITEM 68. ESTIMATED COST
SECTION VII - POLICE INFORMATION
69a. NAME OF POLICE OFFICER 69b. BADGE NUMBER 69c. TELEPHONE NUMBER
70. PRECINCT OR HEADQUARTERS 71a. PERSON CHARGED WITH ACCIDENT 71b. VIOLATION(S)
STANDARD FORM 91 (2/2004) PAGE 3
SECTION VIII - EXTRA DETAILS
SPACE FOR DETAILED ANSWERS. INDICATE SECTION AND ITEM NUMBER FOR EACH ANSWER. IF MORE SPACE IS NEEDED, CONTINUE ITEMS ON PLAIN BOND
PAPER.
PRIVACY ACT STATEMENT
The information on this form is subject to the Privacy Act of 1974 (5 U.S.C. section 552a). Authority to collect the information is Title 40
U.S.C. Section 491 and the title 31 U.S.C. Section 7701. The formation is required by federal Government agencies to administer motor
vehicle programs, including maintaining records on accidents involving privately owned and Federal fleet vehicles,and collecting
accident claims resulting from accidents. Federal employees, and employees under contract, will use the information only in the
performance of their official duties. Routine uses of the collected information may include disclosures to: appropriate Federal, State, or
local agencies or contractors when relevant to civil, criminal, or regulatory investigations or prosecutions; the Office of personnel
Management and the General Accounting Office for program evaluation purposes; a Member of Congress or staff in response to a
request for assistance by the individual of record; another Federal agency, including the Department of Treasury and Justice, or a court
under judicial proceedings; agency Inspectors General in conducting audits; private insurance and the collection agencies (including
agencies under contract to Treasury to collect debt), and to other agency finance offices for federal management and debt collection.
Furnishing the requested information is mandatory, including the Social security Number or Taxpayer's Identification Number(TIN) for
use as a unique identifier to ensure accurate identification for individuals or firms in the system.
SECTION IX - FEDERAL DRIVER CERTIFICATION
I certify that the information on this form (Sections I thru VII) is correct to the best of my knowledge and belief.
72a. NAME AND TITLE OF DRIVER 72b. DRIVER'S SIGNATURE AND DATE
SECTION X - DETAILS OF TRIP DURING WHICH ACCIDENT OCCURRED
73. ORIGIN 74. DESTINATION
75. EXACT PURPOSE OF TRIP
76. TRIP BEGAN
DATE
TIME (Include AM or PM)
77. ACCIDENT
OCCURRED
DATE
TIME (Include AM or PM)
78. AUTHOURITY FOR THE TRIP WAS GIVEN TO THE OPERATOR
ORALLY
IN WRITING (Explain)
79. WAS THERE ANY DEVIATION FROM DIRECT ROUTE?
NO
YES (Explain)
80. WAS THE TRIP MADE WITHIN ESTABLISHED WORKING HOURS?
YES
NO (Explain)
81. DID THE OPERATOR, WHILE ENROUTE, ENGAGE IN ANY ACTIVITY OTHER
THAN THAT FOR WHICH THE TRIP WAS AUTHORIZED?
NO
YES (Explain)
82. COMPLETED
BY DRIVER'S
SUPERVISOR
a. DID THIS ACCIDENT OCCUR WITHIN THE EMPLOYEE'S SCOPE OF DUTY
YES
NO
b. COMENTS
83a. NAME AND TITLE OF SUPERVISOR 83b. SUPERVISOR'S SIGNATURE AND DATE 83c. TELEPHONE NUMBER
STANDARD FORM 91 (2/2004) PAGE 4
SECTION XI - ACCIDENT INVESTIGATION DATA
84. DID THE INVESTIGATION DISCLOSE CONFLICTING INFORMATION.
85. PERSONS INTERVIEWED
NAME NAMEDATE DATE
a.
b.
c.
d.
86. ADDITIONAL COMMENTS (Indicate section and item number of each comment).
SECTION XII - ATTACHMENTS
87. LIST ALL ATTACHMENTS TO THIS REPORT
SECTION XIII - COMMENTS/APPROVALS
88. REVIEWING OFFICIAL'S COMMENTS
89. ACCIDENT INVESTIGATOR 90. ACCIDENT REVIEWING OFFICIAL
a. SIGNATURE b. DATE
c. NAME (First, middle, last)
d. TITLE
e. OFFICE e. OFFICE
d. TITLE
c. NAME (First, middle, last)
b. DATEa. SIGNATURE
f. OFFICE TELEPHONE NUMBER
f. OFFICE TELEPHONE NUMBER
AREA CODE
AREA CODE
NUMBER NUMBEREXTENSION EXTENSION
NO YES (If checked, explain below.)


