
Fillable Printable U.S. Standard Certificate of Death Form
Fillable Printable U.S. Standard Certificate of Death Form
U.S. Standard Certificate of Death Form
U.S. STANDARD CERTIFICATE OF DEATH
LOCAL FILE NO. STATE FILE NO.
1. DECEDENT’S LEGAL NAME (Include AKA’s if any) (First, Middle, Last)
2. SEX 3. SOCIAL SECURITY NUMBER
4b. UNDER 1 YEAR 4c. UNDER 1 DAY 4a. AGE-Last Birthday
(Years)
Months Days Hours Minutes
5. DATE OF BIRTH (Mo/Day/Yr)
6. BIRTHPLACE (City and State or Foreign Country)
7a. RESIDENCE-STATE 7b. COUNTY 7c. CITY OR TOWN
7d. STREET AND NUMBER 7e. APT. NO. 7f. ZIP CODE
7g. INSIDE CITY LIMITS? □ Yes □ No
8. EVER IN US ARMED FORCES?
□ Yes □ No
9. MARITAL STATUS AT TIME OF DEATH
□ Married □ Married, but separated □ Widowed
□ Divorced □ Never Married □ Unknown
10. SURVIVING SPOUSE’S NAME (If wife, give name prior to first marriage)
11. FATHER’S NAME (First, Middle, Last)
12. MOTHER’S NAME PRIOR TO FIRST MARRIAGE (First, Middle, Last)
13a. INFORMANT’S NAME
13b. RELATIONSHIP TO DECEDENT
13c. MAILING ADDRESS (Street and Number, City, State, Zip Code)
14. PLACE OF DEATH (Check only one: see instructions)
IF DEATH OCCURRED IN A HOSPITAL:
□ Inpatient □ Emergency Room/Outpatient □ Dead on Arrival
IF DEATH OCCURRED SOMEWHERE OTHER THAN A HOSPITAL:
□ Hospice facility □ Nursing home/Long term care facility □ Decedent’s home □ Other (Specify):
15. FACILITY NAME (If not institution, give street & number)
16. CITY OR TOWN , STATE, AND ZIP CODE
17. COUNTY OF DEATH
18. METHOD OF DISPOSITION: □ Burial □ Cremation
□ Donation □ Entombment □ Removal from State
□ Other (Specify):_____________________________
19. PLACE OF DISPOSITION (Name of cemetery, crematory, other place)
20. LOCATION-CITY, TOWN, AND STATE
21. NAME AND COMPLETE ADDRESS OF FUNERAL FACILITY
NAME OF DECEDENT ____________________________________________
For use by physician or institution
To Be Completed/ Verified By:
FUNERAL DIRECTOR:
22. SIGNATURE OF FUNERAL SERVICE LICENSEE OR OTHER AGENT
23. LICENSE NUMBER (Of Licensee)
ITEMS 24-28 MUST BE COMPLETED BY PERSON
WHO PRONOUNCES OR CERTIFIES DEATH
24. DATE PRONOUNCED DEAD (Mo/Day/Yr)
25. TIME PRONOUNCED DEAD
26. SIGNATURE OF PERSON PRONOUNCING DEATH (Only when applicable)
27. LICENSE NUMBER
28. DATE SIGNED (Mo/Day/Yr)
29. ACTUAL OR PRESUMED DATE OF DEATH
(Mo/Day/Yr) (Spell Month)
30. ACTUAL OR PRESUMED TIME OF DEATH
31. WAS MEDICAL EXAMINER OR
CORONER CONTACTED? □ Yes □ No
CAUSE OF DEATH (See instructions and examples)
32. PART I. Enter the chain of events--diseases, injuries, or complications--that directly caused the death. DO NOT enter terminal events such as cardiac
arrest, respiratory arrest, or ventricular fibrillation without showing the etiology. DO NOT ABBREVIATE. Enter only one cause on a line. Add additional
lines if necessary.
IMMEDIATE CAUSE (Final
disease or condition ---------> a._____________________________________________________________________________________________________________
resulting in death) Due to (or as a consequence of):
Sequentially list conditions, b._____________________________________________________________________________________________________________
if any, leading to the cause Due to (or as a consequence of):
listed on line a. Enter the
UNDERLYING C AUSE c._____________________________________________________________________________________________________________
(disease or injury that Due to (or as a consequence of):
initiated the events resulting
in death) LAST d._____________________________________________________________________________________________________________
Approximate
interval:
Onset to death
_____________
_____________
_____________
_____________
33. WAS AN AUTOPSY PERFORMED?
□ Yes □ No
PART II. Enter other significant conditions contributing to death but not resulting in the underlying cause given in PART I
34. WERE AUTOPSY FINDINGS AVAILABLE TO
COMPLETE THE CAUSE OF DEATH? □ Yes □ No
35. DID TOBACCO USE CONTRIBUTE
TO DEATH?
□ Yes □ Probably
□ No □ Unknown
36. IF FEMALE:
□ Not pregnant within past year
□ Pregnant at time of death
□ Not pregnant, but pregnant within 42 days of death
□ Not pregnant, but pregnant 43 days to 1 year before death
□ Unknown if pregnant within the past year
37. MANNER OF DEATH
□ Natural □ Homicide
□ Accident □ Pending Investigation
□ Suicide □ Could not be determined
38. DATE OF INJURY
(Mo/Day/Yr) (Spell Month)
39. TIME OF INJURY 40. PLACE OF INJURY (e.g., Decedent’s home; construction site; restaurant; wooded area)
41. INJURY AT WORK?
□ Yes □ No
42. LOCATION OF INJURY: State: City or Town:
Street & Number: Apartment No.: Zip Code:
43. DESCRIBE HOW INJURY OCCURRED:
44. IF TRANSPORTATION INJURY, SPECIFY:
□ Driver/Operator
□ Passenger
□ Pedestrian
□ Other (Specify)
45. CERTIFIER (Check only one):
□ Certifying physician-To the best of my knowledge, death occurred due to the cause(s) and manner stated.
□ Pronouncing & Certifying physician-To the best of my knowledge, death occurred at the time, date, and place, and due to the cause(s) and manner stated.
□ Medical Examiner/Coroner-On the basis of examination, and/or investigation, in my opinion, death occurred at the time, date, and place, and due to the cause(s) and manner stated.
Signature of certifier:_____________________________________________________________________________
46. NAME, ADDRESS, AND ZIP CODE OF PERSON COMPLETING CAUSE OF DEATH (Item 32)
To Be Completed By:
MEDICAL CERTIFIER
47. TITLE OF CERTIFIER
48. LICENSE NUMBER
49. DATE CERTIFIED (Mo/Day/Yr)
50. FOR REGISTRAR ONLY- DATE FILED (Mo/Day/Yr)
51. DECEDENT’S EDUCATION-Check the box
that best describes the highest degree or level of
school completed at the time of death.
□ 8th grade or less
□ 9th - 12th grade; no diploma
□ High school graduate or GED completed
□ Some college credit, but no degree
□ Associate degree (e.g., AA, AS)
□ Bachelor’s degree (e.g., BA, AB, BS)
□ Master’s degree (e.g., MA, MS, MEng,
MEd, MSW, MBA)
□ Doctorate (e.g., PhD, EdD) or
Professional degree (e.g., MD, DDS,
DVM, LLB, JD)
52. DECEDENT OF HISPANIC ORIGIN? Check the box
that best describes whether the decedent is
Spanish/Hispanic/Latino. Check the “No” box if
decedent is not Spanish/Hispanic/Latino.
□ No, not Spanish/Hispanic/Latino
□ Yes, Mexican, Mexican American, Chicano
□ Yes, Puerto Rican
□ Yes, Cuban
□ Yes, other Spanish/Hispanic/Latino
(Specify) __________________________
53. DECEDENT’S RACE (Check one or more races to indicate what the
decedent considered himself or herself to be)
□ White
□ Black or African American
□ American Indian or Alaska Native
□ Asian Indian
(Name of the enrolled or principal tribe) _______________
□ Chinese
□ Filipino
□ Japanese
□ Korean
□ Vietnamese
□ Other Asian (Specify)__________________________________________
□ Native Hawaiian
□ Guamanian or Chamorro
□ Samoan
□ Other Pacific Islander (Specify)_________________________________
□ Other (Specify)___________________________________________
54. DECEDENT’S USUAL OCCUPATION (Indicate type of work done during most of working life. DO NOT USE RETIRED).
To Be Completed By:
FUNE RAL DIRECTOR
55. KIND OF BUSINESS/INDUSTRY
REV. 11/2003
MEDICAL CERTIFIER INSTRUCTIONS for selected items on U.S. Standard Certificate of Death
(See Physicians’ Handbook or Medical Examiner/Coroner Handbook on Death Registration for instructions on all items)
ITEMS ON WHEN DEATH OCCURRED
Items 24-25 and 29-31 should always be completed. If the facility uses a separate pronouncer or other person to indicate that death has taken
place with another person more familiar with the case completing the remainder of the medical portion of the death certificate, the pronouncer
completes Items 24-28. If a certifier completes Items 24-25 as well as items 29-49, Items 26-28 may be left blank.
ITEMS 24-25, 29-30 – DATE AND TIME OF DEATH
Spell out the name of the month. If the exact date of death is unknown, enter the approximate date. If the date cannot be approximated, enter
the date the body is found and identify as date found. Date pronounced and actual date may be the same. Enter the exact hour and minutes
according to a 24-hour clock; estimates may be provided with “Approx.” placed before the time.
ITEM 32 – CAUSE OF DEATH (See attached examples)
Take care to make the entry legible. Use a computer printer with high resolution, typewriter with good black ribbon and clean keys, or print
legibly using permanent black ink in completing the CAUSE OF DEATH Section. Do not abbreviate conditions entered in section.
Part I
(Chain of even ts lead in g directly to death)
•Only one cause should be entered on each line. Line (a)
MUST ALWAYS have an entry. DO NOT leave blank. Additional lines may be added
if necessary.
•If the condition on Line (a) resulted from an underlying condition, put the underlying condition on Line (b) , and so on, until the full sequence is
reported. ALWAYS enter the underlying cause of death on the lowest used line
in Part I.
•For each cause indicate the best estimate of the interval between the presumed onset and the date of death. The terms “unknown ” or
“approximately” may be used. General terms, such as minutes, hours, or days, are acceptable, if necessary. DO NOT leave blank.
•T he terminal event (for example, cardiac arrest or respiratory arrest) should not be used. If a mechanism of death seems most appropriate to
you for line (a), then you must always list its cause(s) on the line(s) below it (for example, cardiac arrest due to coronary artery atherosclerosis or
cardiac arrest due to blunt impact to chest).
• If an organ system failure such as congestive heart failure, hepatic failure, renal failure, or respiratory failure is listed as a cause of death,
always report its etiology on the line(s) beneath it (for example, renal failure due to Type I diabetes mellitus).
•When indicating neoplasms as a cause of death, include the following: 1) primary site or that the primary site is unknown, 2) benign or
malignant, 3) cell type or that the cell type is unknown, 4) grade of neoplasm, and 5) part or lobe of organ affected. (For example, a primary well-
differentiated squamous cell carcinoma, lung, left upper lobe.)
•Always report the fatal injury (for example, stab wound of chest), the trauma (for example, transection of subclavian vein), and impairment of
function (for example, air embolism).
PART II (Other significant conditions)
•Enter all diseases or conditions contributing to death that were not reported in the chain of events in Part I and that did not result in the
underlying cause of death. See attached examples.
•If two or more possible sequences resulted in death, or if two conditions seem to have added together, report in Part I the one that, in your
opinion, most directly caused death. Report in Part II the other conditions or diseases.
CHANGES TO CAUSE OF DEATH
Should additional medical information or autopsy findings become available that would change the cause of death originally reported, the original death
certificate should be amended by the certifying physician by immediately reporting the revised cause of death to the State Vital Records Office.
ITEMS 33-34 - AUTOPSY
•33 - Enter “Yes” if either a partial or full autopsy was performed. Otherwise enter “No.”
•34 - Enter “Yes” if autopsy findings were available to complete the cause of death; otherwise enter “No”. Leave item blank if no autopsy was
performed.
ITEM 35 - DID TOBACCO USE CONTRIBUTE TO DEATH?
Check “yes” if, in your opinion, the use of tobacco contributed to death. Tobacco use may contribute to deaths due to a wide variety of diseases;
for example, tobacco use contributes to many deaths due to emphysema or lung cancer and some heart disease and cancers of the head and
neck. Check “no” if, in your clinical judgment, tobacco use did not contribute to this particular death.
ITEM 36 - IF FEMALE, WAS DECEDENT PREGNANT AT TIME OF DEATH OR WITHIN PAST YEAR?
This information is important in determining pregnancy-related mortality.
ITEM 37 - MANNER OF DEATH
•Always check Manner of Death, which is important: 1) in determining accurate causes of death; 2) in processing insurance claims; and 3) in
statistical studies of injuries and death.
•Indicate “Pending investigation” if the manner of death cannot be determined whether due to an accident, suicide, or homicide within the
statutory time limit for filing the death certificate. This should be changed later to one of the other terms.
•Indicate “Could not be Determined” ONLY when it is impossible to determine the manner of death.
ITEMS 38-44 - ACCIDENT OR INJURY – to be filled out in all cases of deaths due to injury or poisoning.
•38 - Enter the exact month, day, and year of injury. Spell out the name of the month. DO NOT use a number for the month. (Remember, the
date of injury may differ from the date of death.) Estimates may be provided with “Approx.” placed before the date.
•39 - Enter the exact hour and minutes of injury or use your best estimate. Use a 24-hour clock.
•40 - Enter the general place (such as restaurant, vacant lot, or home) where the injury occurred. DO NOT enter firm or organization names.
(For example, enter “factory”, not “Standard Manufacturing, Inc.” )
•41 - Complete if anything other than natural disease is mentioned in Part I or Part II of the medical certification, including homicides, suicides,
and accidents. T his includes all motor vehicle deaths. The item must
be completed for decedents ages 14 years or over and may be completed
for those less than 14 years of age if warranted. Enter “Yes” if the injury occurred at work. Otherwise enter “No”. An injury may occur at work
regardless of whether the injury occurred in the course of the decedent’s “usual” occupation. Examples of injury at work and injury not at work
follow:
Injury at work Injury not at work
Injury while working or in vocational training on job premises
Injury while engaged in personal recreational activity on job premises
Injury while on break or at lunch or in parking lot on job premises
Injury while a visitor (not on official work business) to job premises
Injury while working for pay or compensation, including at home
Homemaker working at homemaking activities
Injury while working as a volunteer law enforcement official etc.
Student in school
Injury while traveling on business, including to/from business contacts Working for self for no profit (mowing yard, repairing own roof, hobby)
Commuting to or from work
•42 - Enter the complete address where the injury occurred including zip code.
•43 - Enter a brief but specific and clear description of how the injury occurred. Explain the circumstances or cause of the injury. Specify
type of gun or type of vehicle (e.g., car, bulldozer, train, etc.) when relevant to circumstances. Indicate if more than one vehicle involved;
specify type of vehicle decedent was in.
•44 -Specify role of decedent (e.g. driver, passenger). Driver/operator and passenger should be designated for modes other than motor vehicles
such as bicycles. Other applies to watercraft, aircraft, animal, or people attached to outside of vehicles (e.g. surfers).
Rationale
: Motor vehicle accidents are a major cause of unintentional deaths; details will help determine effectiveness of current safety features
and laws.
REFERENCES
For more information on how to complete the medical certification section of the death certificate, refer to tutorial at http://www.TheNAME.org and
resources including instructions and handbooks available by request from NCHS, Room 7318, 3311 Toledo Road, Hyattsville, Maryland 20782-
2003 or at www.cdc.gov/nchs/about/major/dvs/handbk.htm
REV. 11/2003
Cause-of-death – Background, Examples, and Common Problems
Accurate cause of death info rmation is important
•to the public health community in evaluating and im proving the health of all citizens, and
•often to the family, now and in the future, and to the person settling the decedent’s estate.
The cause-of-death section consists of two parts. Part I is for reporting a chain of events leading directly to death, with the immediat e cause of death (the final disease, injury, or complication directly causing death) on
line a and the underlying cause of death (the disease or injury that initiated the chain of events that led directly and inevitably to death) on the lowest used line. Part II is for reporting all other significant diseases,
conditions, or injuries that contributed to death but which did not result in the underlying ca use of death given in Part I. The cause-of-death information should be YOUR best medical OPINION. A condition can be
listed as “probable” even if it has not been definitively diagnosed.
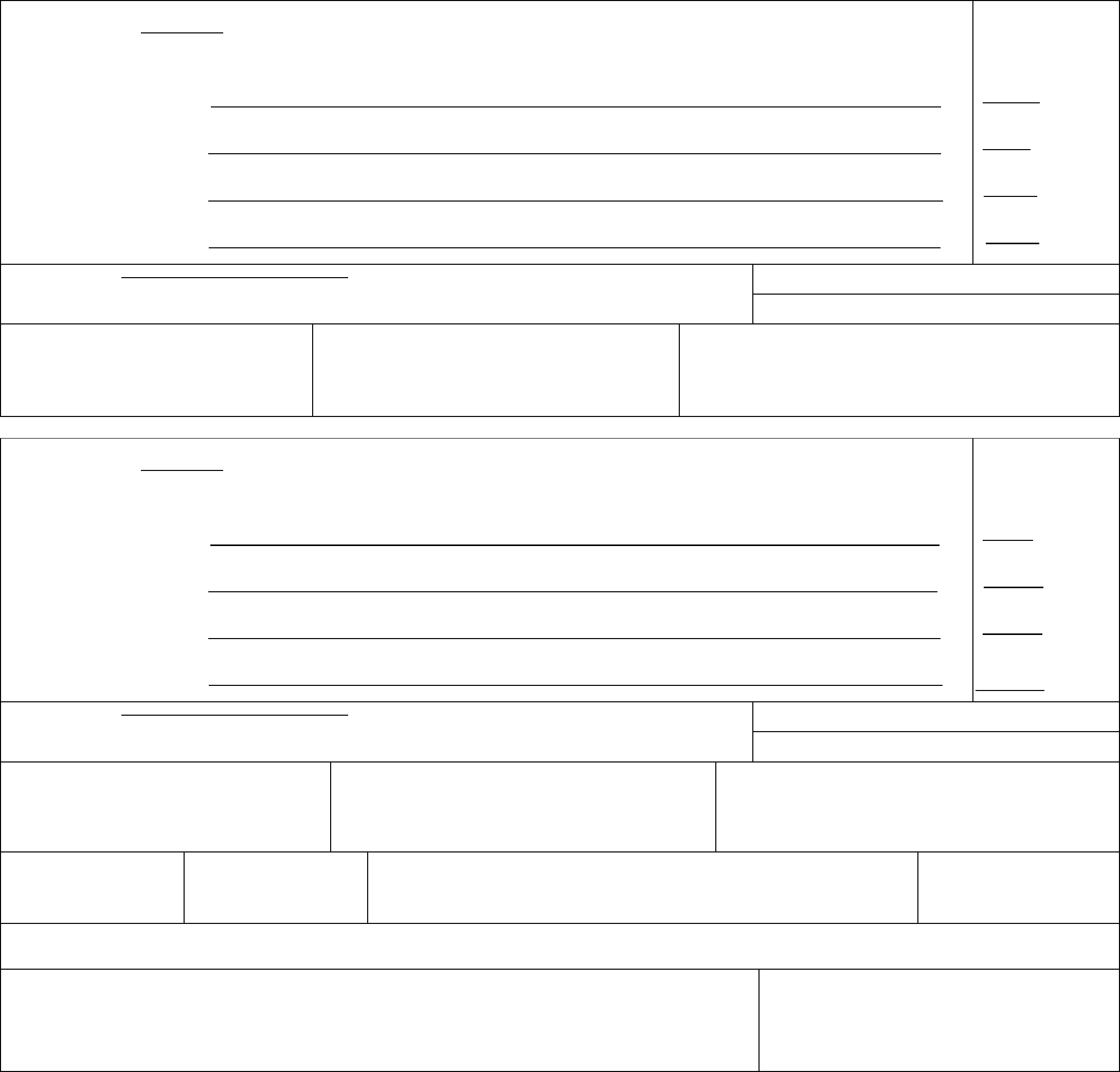
Examples of properly completed medical certifications
CAUSE OF DEATH (See instructions and examples)
32. PART I. Enter the chain of events--diseases, injuries, or complications--that directly caused the death. DO NOT enter terminal events such as cardiac
arrest, respiratory arrest, or ventricular fibrillation without showing the etiology. DO NOT ABBREVIATE. Enter only one cause on a line. Add additional
lines if necessary.
IMMEDIATE CAUSE (Final
disease or condition ---------> a. Rupture of myocardium __________________________________________________________________________________
resulting in death) Due to (or as a consequence of):
Sequentially list conditions, b. Acute myocardial infarction_______________________________________________________________________________
if any, leading to the cause Due to (or as a consequence of):
listed on line a. Enter the
UNDERLYING C AUSE c. Coronary artery thrombosis_______________________________________________________________________________
(disease or injury that Due to (or as a consequence of):
initiated the events resulting
in death) LAST d.
Atherosclerotic coronary artery disease__________________________________________________________________
Approximate interval:
Onset to death
Minutes
6 days
5 years
7 years
33. WAS AN AUT OPSY PERFORMED?
■ Yes No
PART II. Enter other significant conditions contributing to death but not resulting in the underlying cause given in PART I
Diabetes, Chronic obstructive pulmonary disease, smoking
34. WERE AUTOPSY FINDINGS AVAILABLE TO
COMPLETE THE CAUSE OF DEATH? ■ Yes No
35. DID TOBACCO USE CONTRIBUTE TO DEATH?
■ Yes Probably
No Unknown
36. IF FEMALE:
■ Not pregnant within past year
Pregnant at time of death
Not pregnant, but pregnant within 42 days of death
Not pregnant, but pregnant 43 days to 1 year before death
Unknown if pregnant within the past year
37. MANNE R OF DEATH
■ Natural Homicide
Accident Pend ing Investigatio n
Suicide Could not be determined
CAUSE OF DEATH (See instructions and examples)
32. PART I. Enter the chain of events--diseases, injuries, or complications--that directly caused the death. DO NOT enter terminal events such as cardiac
arrest, respiratory arrest, or ventricular fibrillation without showing the etiology. DO NOT ABBREVIATE. Enter only one cause on a line. Add additional
lines if necessary.
IMMEDIATE CAUSE (Final
disease or condition ---------> a. Aspiration pneumonia_______________________________________________________________
resulting in death) Due to (or as a consequence of):
Sequentially list conditions, b. Complications of coma___________________________________________________________________________________
if any, leading to the cause Due to (or as a consequence of):
listed on line a. Enter the
UNDERLYING C AUSE c. Blunt force injuries________________________________________________________________________________________
(disease or injury that Due to (or as a consequence of):
initiated the events resulting
in death) LAST d. Motor vehicle accident____________________________________________________________________________________
Approximate interval:
Onset to death
2 Days
7 weeks
7 weeks
7 weeks
33. WAS AN AUT OPSY PERFORMED?
■ Yes No
PART II. Enter other significant conditions contributing to death but not resulting in the underlying cause given in PART I
34. WERE AUTOPSY FINDINGS AVAILABLE TO
COMPLETE THE CAUSE OF DEATH? ■ Yes No
35. DID TOBACCO USE CONTRIBUTE TO DEATH?
Yes Probably
■ No Unknown
36. IF FEMALE:
Not pregnant with in past year
Pregnant at time of death
Not pregnant, but pregnant within 42 days of death
Not pregnant, but pregnant 43 days to 1 year before death
Unknown if pregnant within the past year
37. MANNE R OF DEATH
Natural Homicide
■ Accident Pending Investigation
Suicide Could not be determined
38. DATE OF INJURY
(Mo/Day/Yr) (Spell Month)
August 15, 2003
39. TIME OF INJURY
Approx. 2320
40. PLACE OF INJURY (e.g., Decedent’s home; construction site; restaurant; wooded area)
road side near state highway
41. INJURY AT WORK?
Yes ■ No
42. LOCATION OF INJURY: State: Missouri City or Town: near Alexandria
Street & Number: mile marker 17 on state route 46a Apartment No.: Zip Code:
43. DESCRIBE HOW INJURY OCCURRED:
Decedent driver of van, ran off road into tree
44. IF TRANSPORTATION INJUR Y , SPECI FY :
■ Driver/Operator
Passenger
Pedestrian
Other (Specify)
Common problems i n death certification
The elderly decedent should have a clear and distinct etiological sequence for cause of death, if possible. Terms such as senescence, infirmity, old age, and advanced age have little value for public health or medical
research. Age is recorded elsewhere on the certificate. When a number of conditions resulted in death, the physician should choose the single sequence that, in his or her opinion, best describes the process leading to
death, and place any other pertinent conditions in Part II. If after caref u l consideration the phy sician cannot det er mine a sequence that ends in death, then the medical examiner or coroner should be consulted about
conducting an investigation or providing assistance in completing the cause of death.
The infant decedent should have a clear and distinct etiological sequence for cause of death, if possible. “Prematurity” should not be entered without explaining the etiology of prematurity. Maternal conditions may have
initiated or affected the sequence that resulted in infant death, and such maternal causes should be reported in addition to the inf ant causes on the infant’s death certificate (e.g., Hyaline membrane disease due to
prematurity, 28 weeks due to placental abruption due to blunt trauma to mother’s abdomen).
When SIDS is suspected, a complete investigation should be conducted, typically by a medical examiner or coroner. If the infant is under 1 year of age, no cause of death is determined after scene investigation, clinical
history is reviewed, and a complete autopsy is performed, then the death can be reported as Sudden Infant Death Syndrome.
When processes such as the following are reported, additional information about the etiology should be reported:
Abscess
Abdominal hemorrhage
Adhesions
Adult respiratory distress syndrome
Acute myocardial infarction
Altered me ntal status
Anemia
Anoxia
Anoxic encephalopathy
Arrhythmia
Ascites
Aspiration
Atrial fibrillation
Bacteremia
Bedridden
Biliary obstruction
Bowel obstruction
Brain in jury
Brain stem hern tion ia
Carcinogenesis
Carcinomatosis
Cardiac arrest
Cardiac dysrhythmia
Cardiomyopathy
Cardiopulmonary arrest
Cellulitis
Cerebral edema
Cerebrovascular accident
Cerebellar tonsillar herniation
Chronic bedridden state
Cirrhosis
Coagulopathy
Compressi on frac tur e
Congestive heart failure
Convulsions
Decubiti
Dehydration
Dementi a (w hen not
otherw e specified) is
Diarrhea
Disseminated intra vascular
coagulopathy
Dysrhythmia
End-stage liver disease
End-stage renal disease
Epidural hematoma
Exsanguination
Failure to thrive
Fracture
Gangrene
Gastrointesti nal he morrhage
Heart failure
Hemothorax
Hepatic failure
Hepatitis
Hepatorenal syndrome
Hyperglycemia
Hyperkalemia
Hypovolemic shock
Hyponatremia
Hypotension
Immunosuppression
Increased intra cranial pressure
Intra cranial hemorrhage
Malnutrition
Metabolic ence ph al op athy
Multi-organ failure
Multi-system organ failure
Myocardial infarction
Necrotizing soft-tissue infection
Old age
Open (o r closed) head injury
Paralysis
Pancytopenia
Perforated gallbladder
Peritonitis
Pleural effusions
Pneumonia
Pulmonary arrest
Pulmonary edema
Pulmonary embolism
Pulmonary insufficiency
Renal fail ur e
Respiratory arrest
Seizures
Sepsis
Septic shock
Shock
Starvation
Subdural hematoma
Subarachnoid hemorrhage
Sudden death
Thrombocytopenia
Uncal herniation
Urinary tract inf ection
Ventricular fibrillation
Ventricular tachyc rdia a
Volume depletion
If the certifier is unable to determine the etiology of a process such as those shown above, the process must be qualified as being of an unknown, undetermined, probable, presumed, or unspecified etiology so it is clear
that a distinct etiology was not inadvertently or carelessly omitted.
The following conditions and types of death might seem to be specific or natural but when the medical history is examined further may be found to be complications of an injury or poisoning (possibly occurring long ago).
Such cases should be reported to the medical examiner/coroner.
Asphyxia
Bolus
Choking
Drug or alcohol verdose/drug or o
alcohol abuse
Epidural hematoma
Exsanguination
Fall
Fracture
Hip fracture
Hyperthermia
Hypothermia
Open reducti on o f fract ur e
Pulmonary emboli
Seizure disorder
Sepsis
Subarachnoid hemorrhage
Subdural hematoma
Surgery
Thermal burns/chemical burns
REV. 11/2003

FUNERAL DIRECTOR INSTRUCTIONS for selected items on U.S.
Standard Certificate of Death
(For additional information concerning all items on certificate see Funeral
Directors’ Handbook on Death Registration)
ITEM 1. DECEDENT’S LEGAL NAME
Include any other names used by decedent, if substantially different from the legal name, after the abbreviation AKA (also known as) e.g. Samuel
Langhorne Clemens AKA Mark Twain, but not Jonathon Doe AKA John Doe
ITEM 5. DATE OF BIRTH
Enter the full name of the month (January, February, March etc.) Do not use a number or abbreviation to designate the month.
ITEM 7A-G. RESIDENCE OF DECEDENT (information divided into seven categories)
Residence of decedent is the place where the decedent actually resided. The place of residence is not necessarily the same as “home state” or
“legal residence”. Never enter a temporary residence such as one used during a visit, business trip, or vacation. Place of residence during a
tour of military duty or during attendance at college is considered permanent and should be entered as the place of residence. If the decedent
had been living in a facility where an individual usually resides for a long period of time, such as a group home, mental institution, nursing home,
penitentiary, or hospital for the chronically ill, report the location of that facility in item 7. If the decedent was an infant who never resided at
home, the place of residence is that of the parent(s) or legal guardian. Never use an acute care hospital’s location as the place of residence for
any infant. If Canadian residence, please specify Province instead of State.
ITEM 10. SURVIVING SPOUSE’S NAME
If the decedent was married at the time of death, enter the full name of the surviving spouse. If the surviving spouse is the wife, enter her name
prior to first marriage. T his item is used in establishing proper insurance settlements and other survivor benefits.
ITEM 12. MOTHER’S NAME PRIOR TO FIRST MARRIAGE
Enter the name used prior to first marriage, commonly known as the maiden name. This name is useful because it remains constant throughout
life.
ITEM 14. PLACE OF DEATH
The place where death is pronounced should be considered the place where death occurred. If the place of death is unknown but the body is
found in your State, the certificate of death should be completed and filed in accordance with the laws of your State. Enter the place where the
body is found as the place of death.
ITEM 51. DECEDENT’S EDUCATION (Check appropriate box on death certificate)
Check the box that corresponds to the highest level of education that the decedent completed. Information in this section will not appear on
the certified copy of the death certificate. This information is used to study the relationship between mortality and education (which
roughly corresponds with socioeconomic status). This information is valuable in medical studies of causes of death and in programs
to prevent illness and death.
ITEM 52. WAS DECEDENT OF HISPANIC ORIGIN? (Check “No” or appropriate “Yes” box)
Check “No” or check the “Yes” box that best corresponds with the decedent’s ethnic Spanish identity as given by the informant. Note that
“Hispanic” is not a race and item 53 must also be completed. Do not leave this item blank. With respect to this item, “Hispanic” refers to people
whose origins are from Spain, Mexico, or the Spanish-speaking Caribbean Islands or countries of Central or South America. Origin includes
ancestry, nationality, and lineage. There is no set rule about how many generations are to be taken into account in determining Hispanic origin; it
may be based on the country of origin of a parent, grandparent, or some far-removed ancestor. Although the prompts include the major Hispanic
groups, other groups may be specified under “other”. “Other” may also be used for decedents of multiple Hispanic origin (e.g. Mexican-Puerto
Rican). Information in this section will not appear on the certified copy of the death certificate. This information is needed to identify
health problems in a large minority population in the United States. Identifying health problems will make it possible to target public
health resources to this important segment of our population.
ITEM 53. RACE (Check appropriate box or boxes on death certificate)
Enter the race of the decedent as stated by the informant. Hispanic is not a race; information on Hispanic ethnicity is collected separately in item
52. American Indian and Alaska Native refer only to those native to North and South America (i ncluding Central America) and does not include
Asian Indian. Please specify the name of enrolled or principal tribe (e.g., Navajo, Cheyenne, etc.) for the American Indian or Alaska Native. For
Asians check Asian Indian, Chinese, Filipino, Japanese, Korean, Vietnamese, or specify other Asian group; for Pacific Islanders check
Guamanian or Chamorro, Samoan, or specify other Pacific Island group. If the decedent was of mixed race, enter each race (e.g., Samoan-
Chinese-Filipino or White, American Indian). Information in this section will not appear on the certified copy of the death certificate.
Race is essential for identifying specific mortality patterns and leading causes of death among different racial groups. It is also used
to determine if specific health programs are needed in particular areas and to make population estimates.
ITEMS 54 AND 55. OCCUPATION AND INDUSTRY
Questions concerning occupation and industry must be completed for all decedents 14 years of age or older. This information is useful in
studying deaths related to jobs and in identifying any new risks. For example, the link between lung disease and lung cancer and asbestos
exposure in jobs such as shipbuilding or construction was made possible by this sort of information on death certificates. Information in this
section will not appear on the certified copy of the death certificate.
ITEM 54. DECEDENT’S USUAL OCCUPATION
Enter the usual occupation of the decedent. This is not necessarily the last occupation of the decedent. Never enter “retired”. Give kind of work
decedent did during most of his or her working life, such as claim adjuster, farmhand, coal miner, janitor, store manager, college professor, or
civil engineer. If the decedent was a homemaker at the time of death but had worked outside the household during his or her working life, enter
that occupation. If the decedent was a homemaker during most of his or her working life, and never worked outside the household, enter
“homemaker”. Enter “student” if the decedent was a student at the time of death and was never regularly employed or employed full time during
his or her working life. Information in this section will not appear on the certified copy of the death certificate.
ITEM 55. KIND OF BUSINESS/INDUSTRY
Kind of business to which occupation in item 54 is related, such as insurance, farming, coal mining, hardware store, retail clothing, university, or
government. DO NOT enter firm or organization names. If decedent was a homemaker as indicated in item 54, then enter either “own home” or
“someone else’s home” as appropriate. If decedent was a student as indicated in item 54, then enter type of school, such as high school or
college, in item 55. Information in this section will not appear on the certified copy of the death certificate.
NOTE: This recommended standard death certificate is the result of an extensive evaluation process. Information on the process and resulting
recommendations as well as plans for future activities is available on the Internet at: http://www.cdc.gov/nchs/vital_certs_rev.htm.
REV. 11/2003


