
Fillable Printable VA Form 10-583
Fillable Printable VA Form 10-583
VA Form 10-583
CLAIM MEETS THE REQUIREMENT OF VA REGULATION
6. ACTION
5. COMPLETE A OR B AS APPROPRIATE
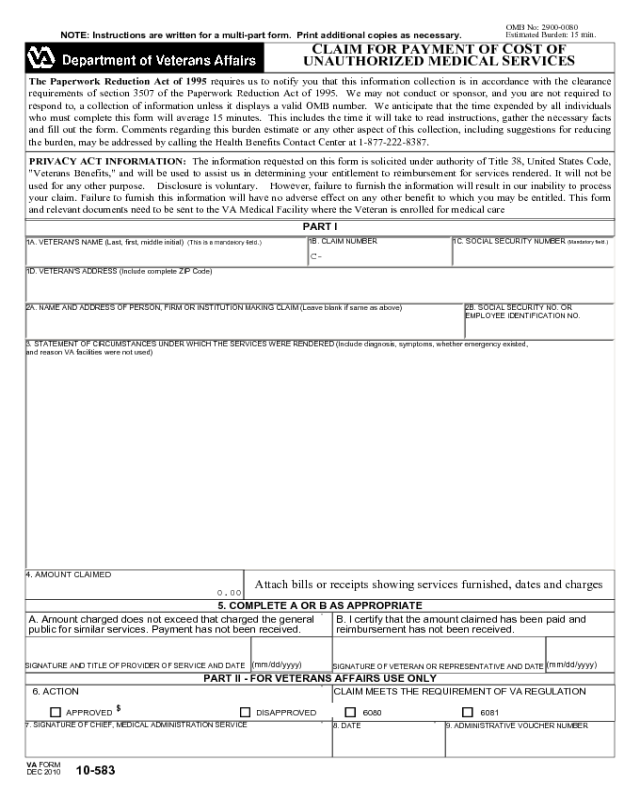
OMB No: 2900-0080
Estimated Burden: 15 min.
CLAIM FOR PAYMENT OF COST OF
UNAUTHORIZED MEDICAL SERVICES
VA FORM
DEC 2010
PRIVACY ACT INFORMATION: The information requested on this form is solicited under authority of Title 38, United States Code,
"Veterans Benefits," and will be used to assist us in determining your entitlement to reimbursement for services rendered. It will not be
used for any other purpose. Disclosure is voluntary. However, failure to furnish the information will result in our inability to process
your claim. Failure to furnish this information will have no adverse effect on any other benefit to which you may be entitled. This form
and relevant documents need to be sent to the VA Medical Facility where the Veteran is enrolled for medical care
PART I
Attach bills or receipts showing services furnished, dates and charges
B. I certify that the amount claimed has been paid and
reimbursement has not been received.
A. Amount charged does not exceed that charged the general
public for similar services. Payment has not been received.
$
10-583
The Paperwork Reduction Act of 1995 requires us to notify you that this information collection is in accordance with the clearance
requirements of section 3507 of the Paperwork Reduction Act of 1995. We may not conduct or sponsor, and you are not required to
respond to, a collection of information unless it displays a valid OMB number. We anticipate that the time expended by all individuals
who must complete this form will average 15 minutes. This includes the time it will take to read instructions, gather the necessary facts
and fill out the form. Comments regarding this burden estimate or any other aspect of this collection, including suggestions for reducing
the burden, may be addressed by calling the Health Benefits Contact Center at 1-877-222-8387.
PART II - FOR VETERANS AFFAIRS USE ONLY
APPROVED DISAPPROVED 6080 6081
NOTE: Instructions are written for a multi-part form. Print additional copies as necessary.
1A. VETERAN'S NAME (Last, first, middle initial) (This is a mandatory field.)
1B. CLAIM NUMBER
1C. SOCIAL SECURITY NUMBER (Mandatory field.)
1D. VETERAN'S ADDRESS (lnclude complete ZIP Code)
2A. NAME AND ADDRESS OF PERSON, FIRM OR INSTITUTION MAKING CLAIM (Leave blank if same as above) 2B. SOCIAL SECURITY NO. OR
EMPLOYEE IDENTIFICATION NO.
3. STATEMENT OF CIRCUMSTANCES UNDER WHICH THE SERVICES WERE RENDERED (Include diagnosis, symptoms, whether emergency existed,
and reason VA facilities were not used)
4. AMOUNT CLAIMED
SIGNATURE AND TITLE OF PROVIDER OF SERVICE AND DATE
(mm/dd/yyyy)
SIGNATURE OF VETERAN OR REPRESENTATIVE AND DATE
(mm/dd/yyyy)
7. SIGNATURE OF CHIEF, MEDICAL ADMINISTRATION SERVICE
8. DATE 9. ADMINISTRATIVE VOUCHER NUMBER
C-
0.00


